Introduction
Ventral hernias are a commonly encountered condition in general surgery with over 600,000 hernia repairs performed annually in the United States.1 Over the past several decades, the volume of ventral hernia repairs performed has nearly doubled with annual costs of almost $10 billion.1 With the increased utilization of minimally invasive surgery across general surgery, the majority of ventral hernia repairs are now performed either using laparoscopic or robotic surgery. These minimally invasive modalities offer several advantages over open repair, including lower rates of wound infections, shorter hospital length of stay, and comparable hernia recurrence rates.2–6
Despite the widespread adoption of laparoscopic ventral hernia repair, recent studies have identified significant gaps in general surgery training for this operation with substantial variability in technical competency among senior residents.7–9 This variability is particularly concerning given the technical complexity of a laparoscopic ventral hernia repair, which requires the integration of core minimally invasive surgical skills with a detailed understanding of abdominal wall anatomy, mesh selection, and intraoperative decision-making. As general surgery residency continues to transition towards competency-based education, ensuring proficiency in laparoscopic ventral hernia repair serves as an essential benchmark for general surgery residency graduates.
Simulation-based curricula provide a cost-effective and reproducible framework of operative skill acquisition; however, data evaluating the efficacy of standardized simulation-based curriculum for laparoscopic ventral hernia repair is limited. This study shares a single-institution experience in implementing a structured laparoscopic ventral hernia curriculum for general surgery residents at an academic institution. We hypothesize that participation in this curriculum will be associated with improved confidence and better performance on key procedural steps of a laparoscopic ventral hernia repair.
Methods
Overview
An Institutional Review Board (IRB) approval for this study was obtained from the Endeavor Health IRB. It was reported in accordance with the ethical standards of institutional research, the Declaration of Helsinki, and the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines.10
A commercially available high-fidelity virtual reality laparoscopic simulator was utilized for this curriculum. A pre-test was conducted prior to a mentored session, where a senior general surgeon worked with the resident to refine their foundational understanding of laparoscopic ventral hernia repair as well as provide individualized feedback on resident performance. A post-test was administered after allowing the resident to practice independently using the laparoscopic simulator during their general surgery rotation. The primary outcome measured were self-reported confidence and performance as well as evaluator-assessed performance on several key steps of a laparoscopic ventral hernia repair on the simulator. Statistical analysis was performed to compare differences in pre- and post-mentor session test scores among general surgery residents.
Participants
General surgery residents from 2014 to 2022 across several postgraduate years (PGY), including PGY 2 through 5, were included in this study. Residents across post-graduate years (PGY) 2 – 5 participated in this rotation during a core general surgery rotation. Because participation in this simulation curriculum was embedded within a required core general surgery rotation for all PGY 2-5 residents, the inclusion of a non-participating control group was not feasible without selectively withholding a mandated education experience from a subset of trainees. Participants provided demographic, prior exposure, sleep/fatigue information, and video gaming history.
Intervention
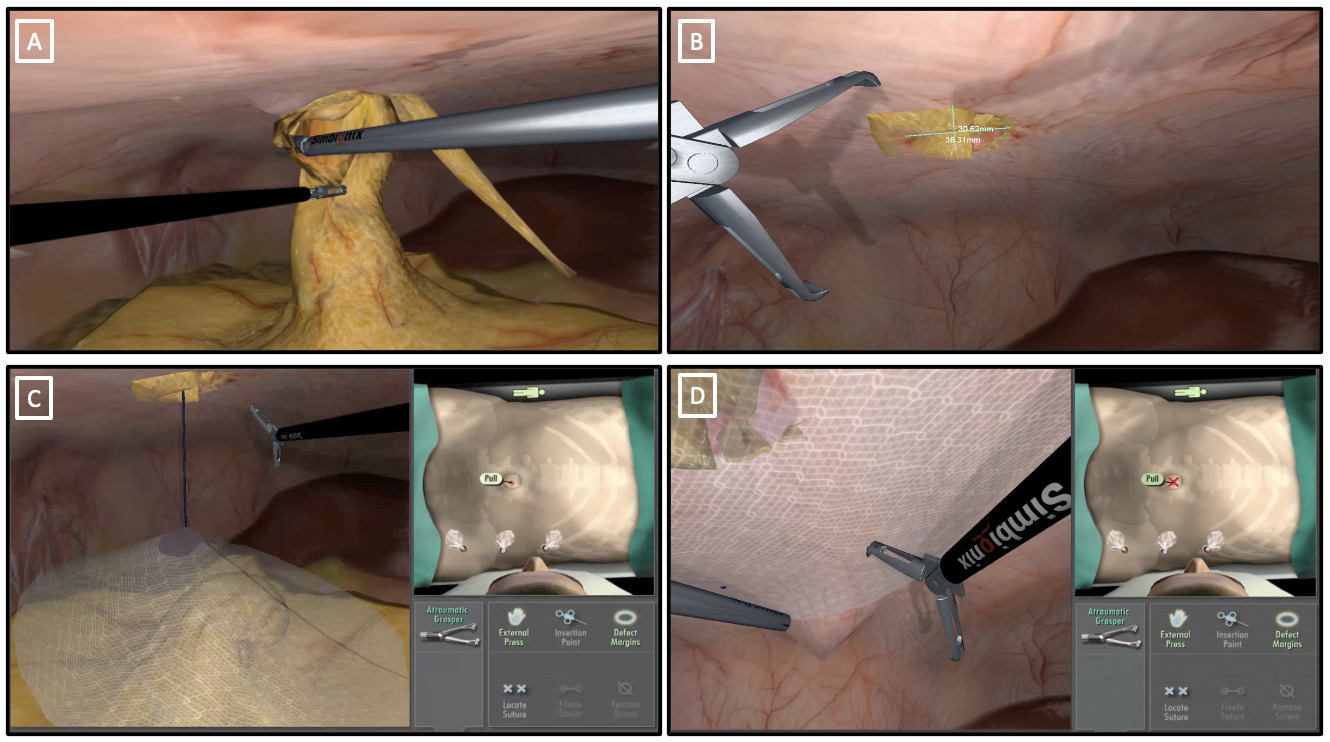
For this curriculum, the Surgical Science Sweden (previously Simbionix) LAP Mentor simulator was used.11 This is a high-fidelity virtual reality simulator that provides tactile feedback, highly realistic and detailed graphics, and an immersive training experience in several different general surgical operations. In particular, residents were instructed to complete a virtual-reality repair of a 3 x 3 cm umbilical hernia with Intraperitoneal Onlay Mesh (IPOM) placement. The module began with the residents inserting their instruments into the trocar, which resulted in the virtual instruments (i.e., atraumatic grasper on the left and Harmonic scalpel on the right) appearing on the screen. After an examination of the abdominal cavity, residents proceeded with adhesioloysis (Figure 1A) followed by reduction of incarcerated contents. Upon completion of this step, the screen prompted the residents to select two spots on the screen to allow the residents to measure the hernia defect (Figure 1B). The residents were then asked to select a mesh on the simulator, with a rectangular, a square and a circular mesh provided as options. Upon selecting a mesh, the residents were asked to select the size of mesh with the following options provided: 10 cm x 15 cm, 15 cm x 20 cm, 20 cm x 25 cm, and 25 cm x 35 cm. After size selection, the screen prompted the residents to select one of two options: placing transfascial sutures later or placing sutures now. Following this selection, they were asked to indicate suture placement and positioning within the mesh. The simulation did not however prompt residents to practice placing transfascial sutures virtually. A video was then played in the simulator, demonstrating proper technique of rolling the mesh prior to insertion into the abdominal cavity. The virtual instruments were once again activated, allowing the residents to interact with the mesh (Figure 1C). Lastly, the residents were then expected to properly position, orient, and fix the mesh to cover the hernia defect adequately prior to the completion of the module. The virtual reality simulator allowed to select different types of surgical instruments, including suture passers, which were utilized to fix the mesh over the hernia defect.
_adhesiolys.png)
Prior to the pre-test, residents received a brief overview of the simulator, which included a discussion on the purpose of the simulator, instrument handling, navigation between instruments, and application of energy sources. The residents were then asked to complete and were evaluated on several technical tasks, including trocar placement, adhesiolysis, mesh selection, and mesh fixation. The resident performance in these tasks was evaluated both by the resident and an expert evaluator using Likert scale surveys. Because the simulation trainer had pre-inserted trocars and instrument, trocar placement was evaluated by a separate questionnaire that assessed residents’ understanding of the number, size, and location of trocar placement for the ventral hernia repair. Residents were also evaluated on adhesioloysis, where the evaluator examined their ability to perform adequate and safe dissection of adhesions with appropriate use of energy sources to clearly delineate hernia defect. Here, residents were scored from 1 (unable to identify appropriate planes to perform safe and adequate dissection, significant unnecessary bleeding, unsafe use of energy sources) to 5 (precisely identify planes to expertly perform safe and adequate dissection, complete maintenance of hemostasis, and appropriate use of energy sources). The evaluators also examined the ability of residents to estimate size and shape of mesh by accurate measurement of the hernia defect with adequate overlap. Residents were scored from 1 (unable to estimate size and shape of mesh, requiring extensive verbal assistance) to 5 (precise estimation of size and shape of the mesh without prompting). Next, the evaluator examined the residents’ ability to introduce and achieve proper orientation and positioning of the mesh, and the residents were scored from 1 (unable to introduce and achieve proper orientation and positioning of the mesh despite verbal prompts) to 5 (expertly able to introduce and achieve proper orientation and positioning of the mesh). Proper fixation of the mesh was also evaluated, ensuring at least 3 cm overlap on each side, flat placement of mesh, using contralateral hand to apply tacks to the edge of the mesh at 1-cm intervals to prevent exposure of its adhesiogenic surface). In this portion of the simulation, residents were scored from 1 (unable to safely and properly perform fixation of the mesh despite verbal prompts) to 5 (expertly able to perform safe and proper fixation of the mesh). Overall knowledge and autonomy to choose proper instruments were also tested, with residents being scored from 1 (lack of knowledge and autonomy to choose appropriate instruments, requiring extensive guidance) to 5 (adequate knowledge and complete autonomy to choose appropriate instruments). Lastly, operator’s overall competence for optimal and organized performance with satisfactory results were also tested, with residents being scored from 1 (requiring extensive guidance for every step of the procedure) to 5 (expertly completing the procedure without prompting). There were no set minimum scores on the simulator that the residents had to achieve on each exercise. Additionally, the residents also score their confidence in performing each task on a Likert scale survey, with 1 being “Strongly Disagree” to being able to confidently perform a given step and 5 being “Strongly Agree.”
Prior to the participation, all evaluators completed a structured calibration protocol to ensure scoring consistency. During this training phase, evaluators were blinded to trainee identity and independently scored pre-recorded pre- and post-test videos of a hernia repair simulation. A weighted Kappa statistic of ≥ 0.75 was required to pass evaluator training and proceed to study participation. A total of seven evaluators participated across the study period, each having successfully completed the credentialing process prior to assessing any study participants. During the study, the evaluators were not blinded to the pre- versus post-test designation, as this was inherent to the study design.
During the rotation, the residents met with a single experienced general surgeon for an hour-long mentor session where the resident went through the module again while receiving feedback on each discrete step of the virtual reality ventral hernia simulation as well as education on how to properly perform the hernia repair. This portion of the curriculum also included a brief didactic discussion addressing mesh characteristics, including adhesion barrier properties and material selection, with particular emphasis on overlap planning. Specifically, residents were instructed on minimum overlap of 3-5 cm beyond the hernia defect margins in all directions. At the end of the rotation, the residents are asked to complete a post-test, assessing their technique on the previously tested objectives. Similar to the pre-test, both the resident and the evaluator score resident performance, with the residents also completing a survey gauging their confidence. In a different curriculum at this institution, the authors have implemented a delayed post-post-test to assess knowledge and skill durability beyond the month-long rotation. However, sufficient longitudinal data have not yet accrued to draw meaningful conclusions regarding retention. While delayed post-testing is a valuable adjunct, its implementation is limited by resident participation outside of protected time during a rotation.
Data Collection and Storage
Results from the resident as well as evaluator surveys were obtained immediately after the completion of the module. These results were stored in a secured REDCap® survey, accessible only to staff at the simulation center.
Statistical Analysis
All statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, NC, USA). Continuous variables were presented as mean and standard deviation (SD). Categorical variables were reported as frequencies and percentages. Group comparisons were conducted using Wilcoxon rank-sum tests for independent samples, Wilcoxon signed-rank test for paired data, and chi-square tests for categorical variables. Statistical significance was considered a p-value < 0.05 with two-tailed tests. Differences between pre- and post-test were evaluated to assess for improvement from pre to post-test. The weighted Cohen’s Kappa statistic with quadratic weights was also used to assess agreement between self and evaluator scores. Qualitative survey responses were analyzed using a frequency-based approach by a single rater, with each topic mentioned by residents systematically tallied to identify prevailing themes of strengths, weaknesses, and areas of improvement in this curriculum.
Results
This study included 55 general surgery residents across multiple PGY levels, including 2 PGY-2 (3.6%), 24 PGY-3 (43.6%), 24 PGY-4 (43.6%), and 5 PGY-5 residents (9.1%). Most residents reported prior laparoscopic surgery experience, with 56.4% having performed more than 50 laparoscopic cases as primary surgeon and 76.3% having assisted in more than 50 laparoscopic procedures. While 25.5% of residents had no prior experience performing laparoscopic ventral hernia repair as primary surgeon, 78.2% reported assisting in at least six laparoscopic ventral hernia repair cases. Regarding simulation exposure, 58.2% of residents spent over 10 hours using the Fundamentals of Laparoscopic Surgery (FLS) trainer, whereas only 5.5% reported no prior exposure. A history of video gaming was reported by 50.9% of residents, with 18.2% currently playing video games. Additionally, 54.5% of residents had performed greater than 6 open ventral hernia repairs as primary surgeons, with 81.8% reporting assisting in greater than 6 open ventral hernia repairs.
Residents demonstrated significant improvement in self-assessed performance following completion of the curriculum, with an increase in total score (maximum achievable score of 35) from pre-test to post-test (25.1 vs. 30.0; p<0.0001), as well as significant improvement across all individual assessment domains. Similarly, overall evaluator-assessed scores improved significantly after the curriculum (22.7 vs. 31.1; p<0.0001) (Table 1). Completion of this simulation-based curriculum was also associated with increased resident confidence, with total confidence survey scores improving from 36.4 to 43.1 (p<0.0001) (Table 2).
On pre-test evaluation, residents consistently rated their performance higher than evaluators across several domains, including mesh introduction (3.7 vs. 3.0; p<0.0001), mesh fixation (3.3 vs. 2.8; p<0.006), instrument use knowledge (3.8 vs. 3.2; p<0.0001), overall competence (3.4 vs. 3.1; p=0.01), and the total score (25.1 vs. 22.7; p=0.0002). In contrast, post-test evaluations demonstrated higher evaluator scores compared to resident self-assessed scores in mesh introduction (4.6 vs. 4.3; p=0.0161) and overall competence (4.4 vs. 4.1; p=0.0081). There were no significant differences between resident and evaluator post-test total scores (Table 3). The weighted Cohen’s Kappa statistic revealed slight to fair agreement in all evaluated components of the hernia repair.
Perceived difficulty of the module was not associated with differences in post-test scores or degree of improvement (Supplemental Table 1). Similarly, there were no significant differences in post-test scores or improvement between junior and senior residents (Supplemental Table 2). Residents reporting ≥7 hours of sleep demonstrated higher post-test scores on mesh introduction, orientation, and positioning (4.8 vs. 4.4; p=0.01), although no significant differences were observed in total scores or overall improvement (Table 4a). There were also no significant differences in post-test scores between fatigued and non-fatigued residents; however, fatigued residents demonstrated greater improvement in trocar placement (1.1 vs. 0.6; p=0.036), mesh fixation (1.7 vs. 1.0; p=0.035), and total score (9.3 vs. 7.3; p=0.048) (Table 4b).
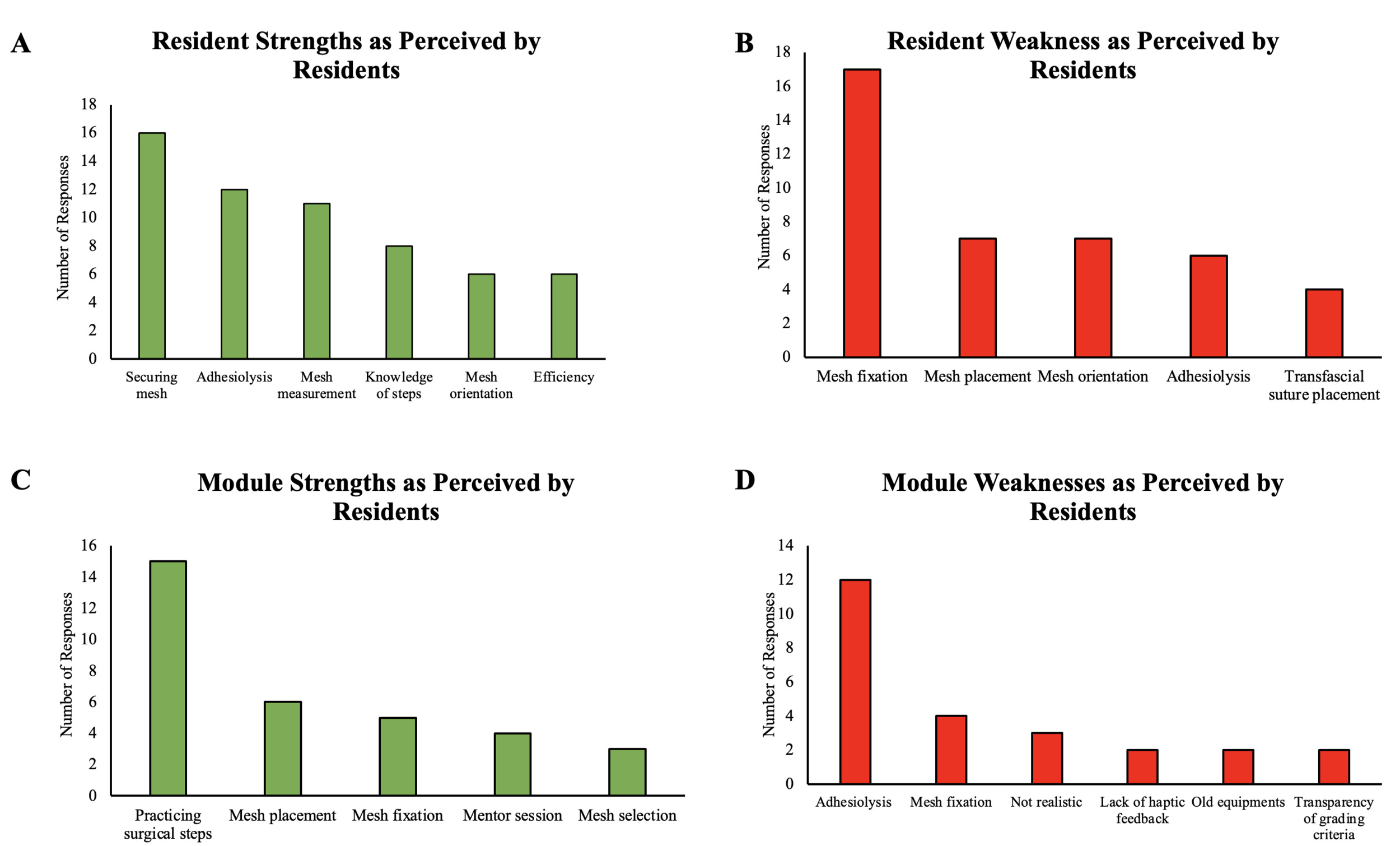
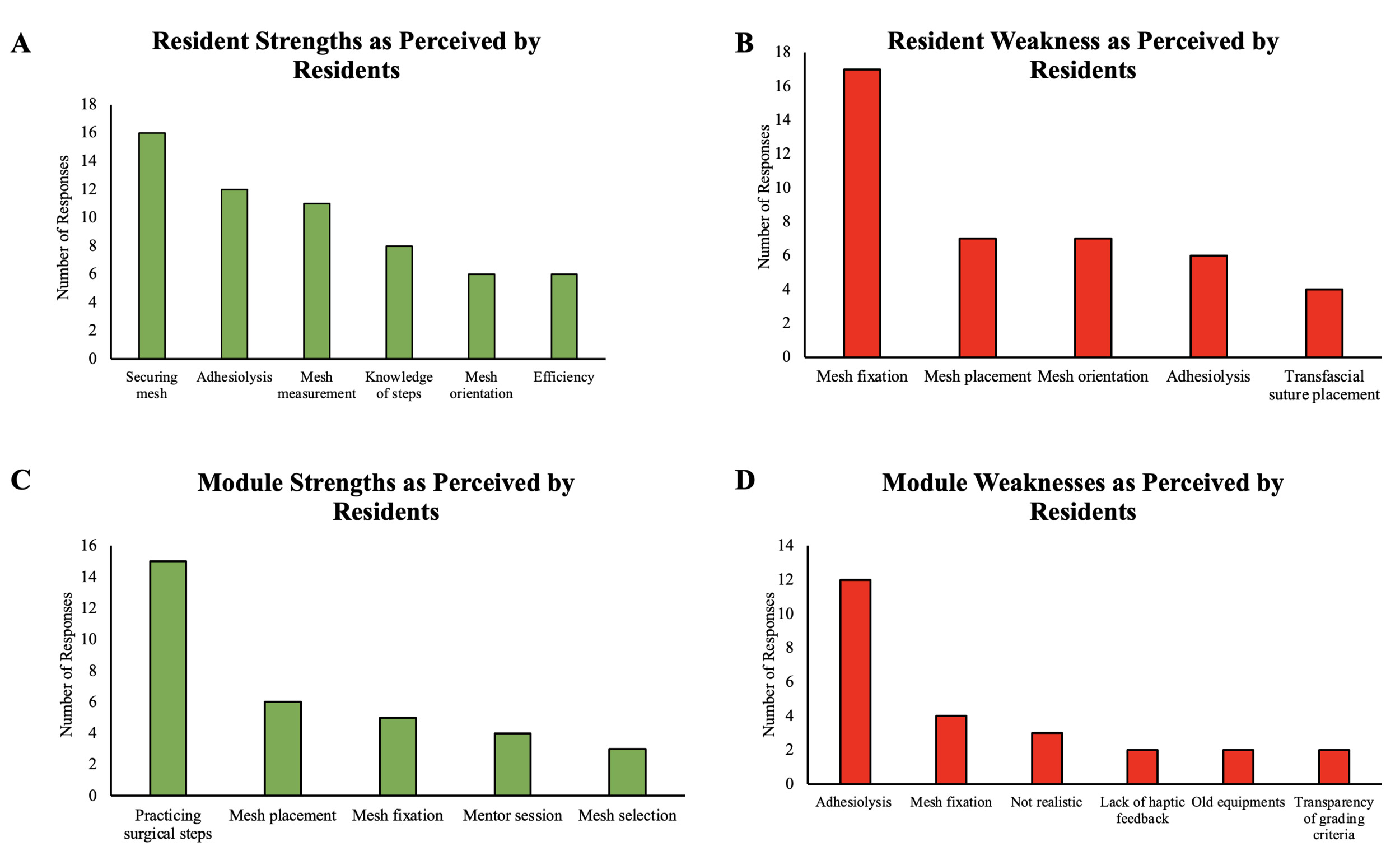
Neither prior experience with laparoscopic or open ventral hernia repair nor video game history was associated with improved performance in this module (Supplemental Tables 3 and 4). Qualitative survey responses revealed that residents perceived their primary strengths to be in mesh securing, adhesiolysis, mesh measurement, procedural knowledge, mesh orientation, and efficiency (Figure 2A). Reported weaknesses included mesh fixation, mesh placement, mesh orientation, adhesiolysis, and transfascial suture placement (Figure 2B). Primary strengths of the module were identified as the opportunity to practice the steps of the operation, mesh placement and fixation, the mentor session, and mesh selection (Figure 2C). Lastly, reported limitations primarily related to specifical technical tasks (adhesiolysis and mesh fixation) and select aspects of realism, haptic feedback, and equipment condition (Figure 2D).
Discussion
This study demonstrated improved technical performance in various domains of a simulated laparoscopic ventral hernia repair, including trocar placement, adhesiolysis, mesh shape and size selection, mesh positioning and fixation, instrument use, and overall competency. These improvements were observed regardless of prior exposure, training level, and perceived difficulty of the module. The increase in post-test score was evident not only in the resident-assessed score, but also in the evaluator-assessed performance, suggesting that residents made meaningful progress throughout the mentored session and the simulation-based curriculum. Collectively, the results underscore the broad educational utility of a simulation-based approach to laparoscopic ventral hernia repair training among general surgery trainees.
Our findings were notable for significant differences in resident-assessed performance and evaluator-assessed performance in several aspects of the pre-test. Specifically, the residents rated themselves higher than the evaluators across several aspects of the simulation in the pre-test, which could reflect the Dunning-Kruger effect, where people with limited competence in a specific domain greatly overestimate their skills.12 The post-test convergence of resident and evaluator scores suggests that the curriculum is effective in aligning trainee self-assessment with objective performance. This finding is consistent with prior surgical education research demonstrating the mentored coaching enhances residents’ abilities to accurately gauge their own skills.13 Specifically, a structured, simulation-based curriculum with individualized mentored coaching can recalibrate resident judgement, reducing tendencies to over- or underestimate performance and foster metacognitive awareness necessary for effective operative proficiency. While the convergence of resident self-evaluation with evaluator ratings at post-test could reflect genuine recalibration following our curriculum, an alternative explanation if evaluator leniency bias, whereby evaluators scored more generously after observing improvement during the curriculum. In the absence of blinded evaluator scoring, these two explanations cannot by fully distinguished. Furthermore, participation in this curriculum was also associated with an improvement in resident confidence that paralleled resident improvement in technical performance. This finding further highlights the well-established role of surgical simulation in fostering skill acquisition, self-efficacy, and technical confidence, factors known to be associated with increasing operative autonomy and readiness for independent surgical practice.14–18
Prior experience in laparoscopic or open ventral hernia repair was not associated with improved performance in the simulation-based module. This finding could be explained by the variability in autonomy and prior experience among residents performing laparoscopic ventral hernia repair. This finding underscores the need for deliberate practice within a structured mentored simulation session for targeted skill acquisition in general surgery. Similarly, video game history, which is often cited to be helpful in surgical skill acquisition,19–22 was not associated with improved performance in this curriculum. While video gaming may require enhanced hand-eye coordination, increased visuospatial awareness, and ability to interpret three-dimensional relationships from a two-dimensional screen, these generalized cognitive and motor skills do not sufficiently transfer to a measurable advantage in complex laparoscopic surgical tasks.
Our study also revealed that increased sleep was associated with improved performance in specific components of laparoscopic ventral hernia repair, namely mesh introduction, orientation, and positioning. This finding aligns with prior literature linking adequate sleep to improved operative performance through improved situational awareness, instrument proficiency, and decision making.23–25 Interestingly, we did not observe differences in overall performance between residents with different sleep durations, a finding that deviates from conventional understanding. Some evidence suggests that sleep and perceived fatigue may not significantly impact skill acquisition or clinical performance in laparoscopic and robotic simulation-based tasks.26,27 Additionally, the absence of differences in overall performance or improvement in our curriculum suggests that the structured, mentored simulation framework is effective across a range of baseline physiologic states, further supporting its generalizability across surgical residents with variable levels of fatigue or sleep.
An unexpected finding was that fatigued residents demonstrated greater improvement in several areas of the simulation including trocar placement, mesh fixation, and overall performance, despite experiencing no difference in absolute total score. While fatigued residents tended towards lower pre-test scores, this difference was not statistically significant, so a floor effect of a lower baseline cannot be used as a definitive explanation. An alternative explanation may be that a controlled simulation environment may mitigate some of the negative effects of fatigue observed in the clinical setting. Simulation-based modules may allow fatigued residents to engage more fully with deliberate practice. This phenomenon warrants further investigation, but our study supports the notion that surgical simulation provides a valuable educational buffer against variability in surgical resident fatigue. Additionally, the threshold used to define fatigue (≥ 3 on a 1-5 Likert scale) was selected a priori to maximize group distribution and analytical power. When a more conservative cutoff (≥4 on a 1-5 Likert scale) was applied, no statistically significant differences were observed between groups; however, this reclassification yielded only three fatigued residents, rendering the comparison underpowered and precluding any meaningful interpretation. We therefore implemented the original threshold to preserve statistical power while acknowledging that the Will-Rogers effect cannot be entirely excluded as a contributor to the observed differences.
As the field of abdominal wall surgery has evolved, there has been a notable increase in the implementation of robotic surgery for ventral hernia repairs.28–30 This is largely driven by enhanced dexterity, ergonomic advantages, and ease of intracorporeal suturing using the robotic platform. Increasing adoption of robotic surgery in ventral hernia repair may impact resident foundational laparoscopic skills. Our institution is also evaluating resident performance in robotic ventral hernia drills. This initiative aims to address the emerging educational need of providing structured, deliberate practice in abdominal wall hernia repair. Collectively, these efforts reflect a comprehensive approach to surgical education, one that adapts with the evolving landscape of general surgery.
This study has several notable strengths. First, it includes a diverse cohort of general surgery residents from a variety of postgraduate years. Second, conducting this study using a commercially available, high-fidelity simulation model was cost-effective, given the model’s easy operability and capacity of repeated use across multiple residents. Third, through the mentored sessions, we targeted a technically complex skill while providing individualized feedback, which resulted in better performance and understanding of principles of laparoscopic ventral hernia repair. Fourth, the pre- and post-test were standardized, allowing for meaningful comparisons between residents across various years of training. Fifth, the study evaluated for modifiable factors such as sleep, fatigue, and prior ventral hernia repair to minimize fatigue and experience-related confounder. Lastly, evaluator scoring was strengthened by standardized rater training, which helped promote consistency in grading and reduce inter-rater variability from one session to next.
The findings of this study must be interpreted in the context of its limitations. This is a single institution curriculum, which could limit the generalizability of our results. Importantly, this study lacks a control group, and therefore improvements in post-test performance cannot be attributed exclusively to the simulation curriculum. Natural learning, test familiarity, and regression to the mean represent alternative explanations that cannot be excluded. Additionally, performance in the post-test was assessed within the same month as the pre-test, which limits us from drawing conclusions about long-term durability of skill retention. While the primary comparison between pre- and post-test is sufficiently powered, some of the exploratory subgroup analyses may be underpowered due to the modest sample size. Furthermore, transference of skills from the simulation-based session to the operating room remains unknown. While our group has previously investigated skill transference from simulation to the operating room, this remains among the most methodologically demanding objectives in surgical education research.31 Meaningful conclusions require sustained longitudinal follow-up, sufficient operative volume, and protected time beyond the rotation, barriers that our prior work took nearly a decade to overcome. Baseline information regarding sleep, fatigue, and prior experience may have been subject to recall bias. Additionally, the qualitative survey revealed that residents cited several limitations of the simulation, including older equipment, limited haptic feedback, and reduced realism. These factors may have influenced technical performance by affecting instrument ergonomics, tactile sensation, and visual cues compared to contemporary operative environment. Thematic analysis was conducted by a single reviewer, and the absence of independent dual coding or formal inter-rater reliability assessment is another limitation. These findings should be interpreted as exploratory, and future studies should include qualitative methodology such as independent coding and kappa statistics to validate identified themes.
Conclusion
Simulation-based laparoscopic ventral hernia repair curriculum significantly improves resident technical performance, confidence, and alignment between self-assessment and objective performance. These findings support the integration of structured, mentored simulation into general surgery may serve as a valuable adjunct to surgical education. Future studies should prospectively collect intraoperative data using validated assessment tools with blinded faculty evaluation before and after curriculum completion to evaluate the transfer of simulation-acquired skills to the operating room. For robotic surgery, metrics available in the robotic platform may be utilized to address the intraoperative assessment gap. Additional studies could prospectively track module-specific practice time to better characterize relationship between simulator exposure and technical skill gain. Lastly, future curriculums could build on this module to incorporate more complex skills such as abdominal wall anatomy, reconstruction principles, intracorporeal suturing of fascial defect in ventral hernia repairs.
Acknowledgement
The authors would like to gratefully acknowledge the staff at the Grainger Center for Simulation and Innovation (GCSI) for their invaluable support throughout this study. Their commitment to maintaining a high-quality simulation center along with their logistical coordination were essential to the successful implementation and completion of this work.