


Introduction
Cataract is the leading cause of blindness globally in people over the age of 50, with a greater burden in low- and middle-income countries.1 The prevalence of vision impairment due to cataracts is projected to increase over the next decade as populations grow and age, but effective cataract surgical coverage, defined as the percentage of operable cataracts that have been removed with a good result, was shown to be 36.7% in a 2017 survey of 20 low- and middle-income countries.2 In the face of these challenges, there is widespread agreement on the need to increase the supply of trained ophthalmologists.3
Instruction on safe and efficient cataract surgical techniques is a crucial piece of ophthalmology residency programs, and the traditional model of surgical instruction seats the expert surgeon next to the mentee surgeon. Surgical education, including the number of cases on which student surgeons receive this mentorship, varies widely across the globe. Some ophthalmology residency programs lack adequate mentored, hands-on surgical training,4 and others provide no surgical training at all.5 This gap has been addressed sporadically by teaching physicians traveling to areas where surgical mentorship is needed, but in-person mentorship programs of this nature are limited by travel and time restrictions on mentor surgeons.
With the advent of high-quality audiovisual equipment and high-speed internet connections, distance surgical mentorship has begun to deliver high quality surgical coaching to surgeons anywhere in the world, allowing expert surgeons to teach safe, effective techniques without the cost, time commitment and ecologic footprint involved with travel. Such programs can also provide exposure to a variety of mentors who use a range of techniques and approaches, a feature difficult to achieve using in-person mentoring. Advances in operating visualization systems, such as the Ngenuity 3-D Visualization System (Alcon) and Artevo 800 (Carl Zeiss Meditec), allow for the mentor and the student surgeons to see similar images, and multiple viewers can participate in the live surgical exchange at once.6 Distance surgical mentorship (DSM) has been shown improve subjective ratings of surgical skill in ophthalmology,7 general surgery,8,9 and otolaryngology.10 It has also been shown to increase objective ratings of cataract surgical skill in wet lab simulations.11
Distance surgical mentorship using a high-quality operating visualization system coupled with a teleconferencing solution with low latency can enable excellent, live surgical mentorship. Objective improvements in surgical skill on patients using this technique have not yet been demonstrated. This study aimed to quantify the objective and subjective improvements in cataract phacoemulsification skill resulting from such mentorship.
Methods
This prospective, investigator-masked case series focused on objective and subjective surgical ability in four Honduran ophthalmologists, 3 of whom were within 2 years of residency training graduation and who had completed fewer than 300 total cases. One subject surgeon self-identified as needing improvement in phacoemulsification cataract surgery skill. Ethics approval was obtained from the Institutional Review Board at Hospital General San Felipe (HGSF), where the mentored surgeries were performed, and informed consent was completed with each participant at HGSF for cataract surgery in a teaching institution. Private health information of patients was protected and remained confidential during the execution of this project, and the tenets of the Declaration of Helsinki were followed throughout.
Each surgeon was mentored through 25 cases over 5 weeks between February and July, 2021, performing on average 5 cases a day, one day a week, for a total of 100 cases among the 4 surgeons. The live stream connecting mentors with student surgeons was via teleconference with multiple connections using a modest (10MB) internet connection. In the operating room with the student surgeon was the Ngenuity 3D Vision System (Alcon) connected to a USB Capture HDMI 4K Plus Device, allowing the surgical field image to be displayed in 3D in the teleconference. Also connected to the teleconference in the operating room were a digital cell phone camera displaying the phacoemulsification machine parameters (Infiniti, Alcon) and a touchscreen tablet camera displaying the surgeon’s hands. The mentor was connected to the teleconference through their computer’s camera, allowing visualization of the above cameras and the use of hand gestures, drawings, and photo captures of the live surgery to better guide the student (Figures 1-2). Due to fluctuating internet bandwidth over the course of the study, the mentor surgeons used a mix of 2D and 3D visualization on their computer displays. All cases were recorded, and all surgeries were performed in the ophthalmology operating room of Hospital General San Felipe (HGSF) in Tegucigalpa, Honduras.


Each student surgeon was mentored by 1-2 mentor surgeons per surgical day, and by the end of the 25 cases, each student surgeon had received guidance from 4-6 different mentors. Volunteer mentor surgeons from the US, Mexico, Perú and Honduras participated in this study, and they were a mix of academic, private practice and NGO surgeons with varying levels of teaching experience. The 4 study subjects and all mentors were proficient in English, enabling smooth interactions, and each mentor met with their student surgeon preoperatively and postoperatively to review the cases and important learning points.
Exclusion criteria for the student surgeons were insufficient phacoemulsification training to safely complete cases without supervision, and inability to adhere to the study’s timeline. Patients included were those with visually significant cataract (BCVA of 20/60-20/400) who were medically stable enough to undergo outpatient cataract surgery. Patients were excluded if they had monocular status, complicated or high-risk cataracts, posterior synechiae, poor dilation, or if they were post vitrectomy or felt to be uncooperative.
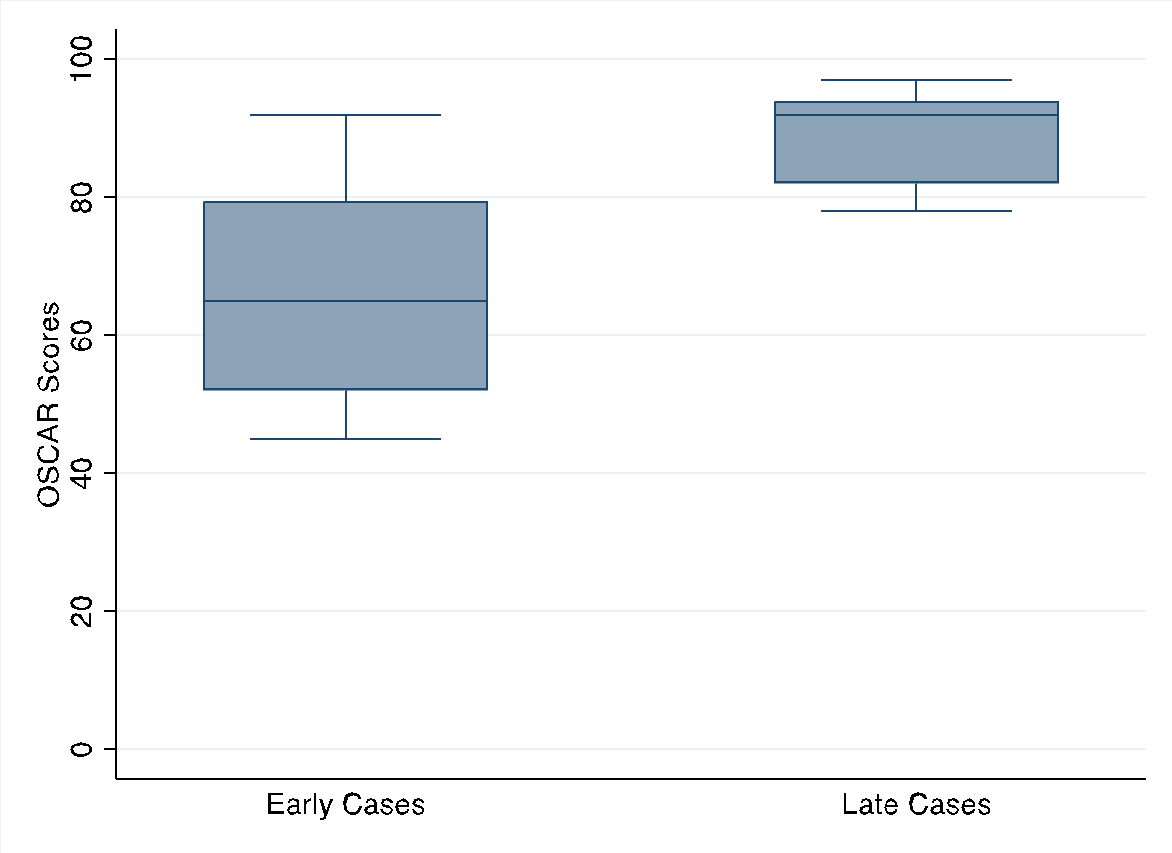
For the primary outcome, an experienced, external, blinded evaluator graded video recordings of cases using the International Council of Ophthalmology - Ophthalmology Surgical Competency Assessment Rubric (OSCAR) scoring system,12 an objective, reliable measure of skill level of surgeons learning phacoemulsification.13 Twenty steps of the procedure are graded on a 1-5 scale for a total possible score of 100. Each surgeon’s first five and final five cases were sent to the external grader, and from those the grader randomly selected three of each five to grade. The primary outcome was the difference in median OSCAR score between the early and the late surgeries among all the surgeons. A Wilcoxan matched pairs sign-rank test was used to compare each surgeon’s OSCAR scores from early and late in the mentorship.
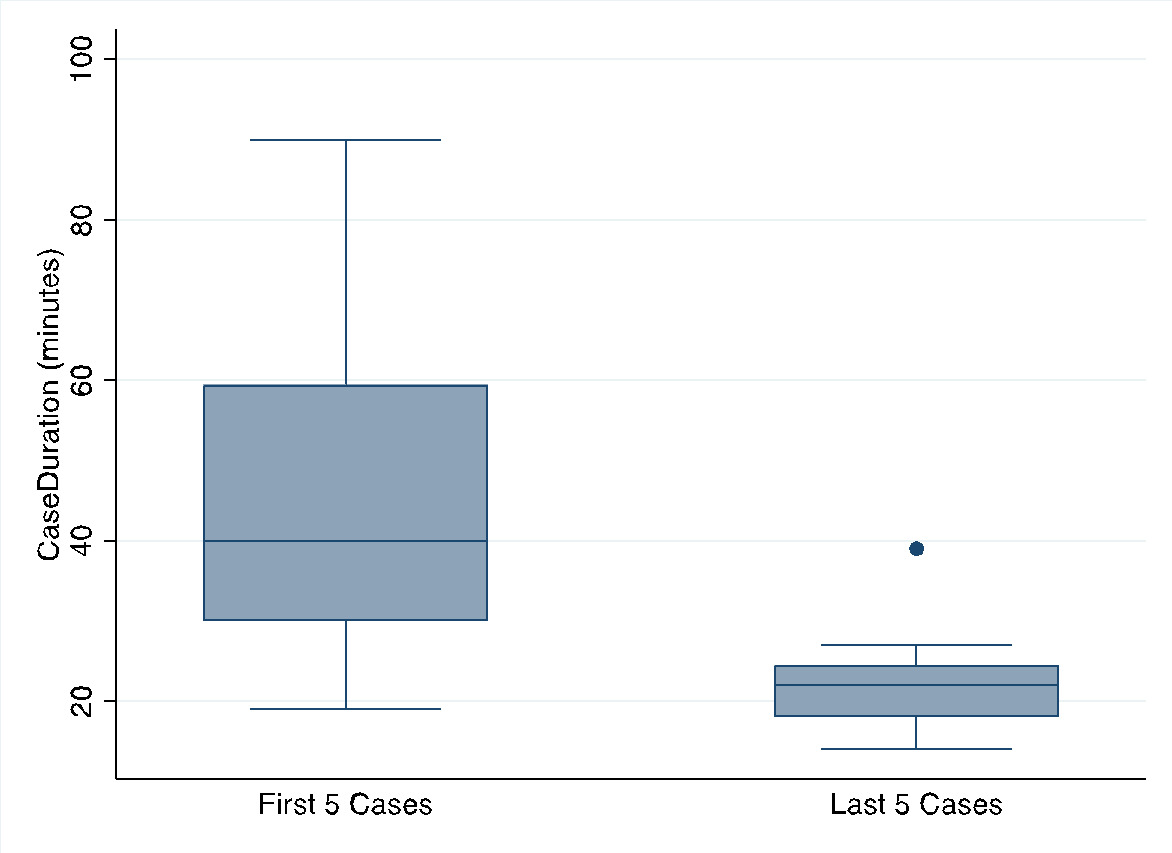
Secondary outcomes were case duration in minutes, complications, cumulative dispersed phacoemulsification energy, and changes in self-rating of surgical skill. Median case duration of the first five and final five cases for each surgeon were matched by surgeon and compared using the Wilcoxan signed rank test. The trend in case duration was evaluated using linear regression of the natural log of mean case duration for each sequential case, 1 through 25. The odds of major complications during the first twelve cases and the final thirteen cases were compared using logistic regression, both crude and adjusted for surgeon and preoperative vision. Median cumulative dispersed energy in the first 5 cases and the final five cases matched by surgeon were compared using a Wilcoxan signed rank test. Self-rating of surgical skill on a scale of 0 to 100 was performed prior to and following the mentorship using a self-administered survey using the same rating scale as the OSCAR score. The change in self-rated surgical skill matched by surgeon was evaluated using the Wilcoxan matched pairs signed rank test. Data analysis was done using Stata software (v 16.1, StataCorp).
Results
A total of 100 cataract surgeries were performed by 4 student surgeons. Mean preoperative logMAR visual acuity ranged from 0.77 to 1.24 (p = 0.42; see Table 1), and major complications occurred in 7 cases (7%; see Table 2.) OSCAR Scores for the group showed a statistically significant increase from a median of 65 (IQR 52-80) for the early surgeries to a median of 92 (IQR 82-94) for the late surgeries (p=0.003, Figure 3a). Median case duration showed a statistically significant decrease from 40 minutes (IQR 30-60) in the first 5 cases to 22 minutes (IQR 18-25) in the final five cases (p=0.007, Figure 3b.) Linear regression of the natural log of the mean of case duration for each sequential case number showed a 3% decrease in mean case duration for every additional mentored case (p < 0.000; 95% CI: 2%-4%.) Logistic regression for the odds of a major complication during the final thirteen cases compared with the first twelve cases showed a crude odds ratio of 0.34 (0.06, 1.89; p=0.22) and an odds ratio of 0.34 (0.05, 1.92; p=0.22) when adjusted for surgeon and preoperative visual acuity (see Table 3.) Median cumulative dispersed energy did not change significantly between the first five and final five cases among all surgeons (14.9 to 15.8, p = 0.90.) On subjective surgical self-rating by the 4 surgeons, median score prior to the mentorship was 63.5 (IQR 55-67) and after the mentorship was 85.5 (82.5-89) (p=0.068.). Improvement was found in self-perceived skill on all procedural steps, with the greatest perceived improvements in constructing the primary incision, capsulorhexis formation and nuclear chopping.

Discussion
The intention of this study was to assess the objective and subjective effect of live streaming, distant surgical mentorship (DSM) on skill in cataract surgery by phacoemulsification. Integral to the study were high quality audio and visualization equipment with low latency, allowing mentor surgeons to have good visualization of the surgical field and enabling live interactions between the student surgeons and the mentors. The student surgeons showed an increase in median OSCAR scores and a decrease in case duration, and the complication rate in this study is comparable to other reports in the literature for phacoemulsification surgeons with comparable experience.14,15
Competency, as measured by case time, complication rate, need for assistance and total phacoemulsification energy, is known to increase with the number of cases a resident has performed.16–18 To our knowledge, this is the first publication reporting the objective and subjective effect of live streaming distance surgical mentorship on cataract surgery competency. Others have previously reported on the concept of distance surgical mentorship and wet lab simulation improvements via this method, but no data on objective improvement in surgical skill has been reported.
Patient safety is of paramount importance when studying surgical education, and it was central to the design and implementation of this study. Compared to traditional, in-person surgical mentorship, DSM does not allow the mentor surgeon to take over the surgery in the face of complications. In-person mentorship is necessary for beginning surgeons, making DSM better suited for surgeons who have already graduated from an ophthalmology residency program and who have some experience with cataract surgery. Additional precautions beyond those typical for surgical training were therefore taken in this study. Student surgeons were selected from among graduates of ophthalmology residency programs who were already performing cataract surgery independently. References were obtained for each surgeon to further validate minimum surgical competency. Patient selection was also carefully considered in the design of this study. Monocular patients, complicated cases, uncooperative patients, and patients with overly dense cataracts were excluded to allow the student surgeon to focus on fundamental surgical techniques.
OSCAR scores and surgical case time are important metrics that can gauge cataract surgical proficiency. The trends of improvement on these metrics seen in this study would possibly continue with further mentoring prior to plateauing, but further studies are needed to assess this relationship.
The major limitation of this study was the small sample size of subject surgeons. Drawing conclusions on the effectiveness of DSM based on the experience of 4 surgeons at different points in their surgical careers is difficult. The main strength of this study is the objective measure of change in surgical skill resulting from the mentorship. No other study to date has quantified the improvements gained through DSM on cataract surgery in patients, and the increase in OSCAR scores and the reduction in surgical times provide valuable quantitative effect estimates.
This study validates the conclusion that DSM using existing technology is effective at increasing objective and subjective surgical skill. High quality video, readily available streaming devices, and a modest internet connection speed can be used in partnership with experienced surgeon mentors to mentor less experienced surgeons. As high-quality equipment becomes more available and as internet speeds increase in the developing world, distance surgical mentoring will enable the dissemination of specialized surgical knowledge without the investment of time and money associated with international travel. Reducing travel also reduces the carbon footprint of surgical mentoring and makes training resistant to disruptions such as the current pandemic. This approach could therefore potentially increase the number of effective surgeons operating globally, allowing qualified eye professionals to begin to address the vast, unmet, global need for surgical eye care. Distance surgical mentoring could represent a powerful new tool in the fight against global blindness.
Acknowledgements
The following surgeons donated time as the volunteer surgical mentors: Daniel Chang, MD; Kevin Waltz, MD, OD; John Berdahl MD, Patricia Sierra, MD; Russell Swan, MD; John Vukich, MD; Marco Robles, MD; Nathan Henson, MD; Matthew Giegengack, MD; Mark Hanson, MD; Anthony Evangelista, MD; Jyoti Gupta, MD; Julia Agopov, MD; Ken Weinlander, MD; Maria Montero, MD; Abner Grijalva, MD.
Dr. David S. Friedman advised on statistical analysis.
Alcon provided the 3D INGENUITY Heads up video equipment used in this project.
Financial disclosure
Kevin Barber is a consultant for Alcon. This study was funded by Alcon through an Investigator Initiated Trial.
The 3D Heads up NGENUITY was provided by Alcon Vision, LLC, Fort Worth, TX, USA.