Introduction
Despite improving gender parity among medical school graduates, surgical specialties remain male-dominated. In 2017, only 20.6% of practicing general surgeons were female, and less than 10% of practicing neurosurgeons, thoracic surgeons, and orthopedic surgeons were female.1 Concerns about gender discrimination are commonly cited by female medical students who ultimately decide against a career in surgery.2,3 These concerns are not unfounded; as gender still limits the training opportunities, professional achievements, career trajectories, and compensation of female surgeons.3 For female medical students, the impact of these inequalities on their choice of specialty may be further compounded by the paucity of female surgeon role models and mentors, relative to their male counterparts.4
Mentorship refers to the tradition of a more experienced individual imparting their knowledge onto a less experienced apprentice to further their professional and personal growth.4,5 Mentorship can profoundly impact a trainee’s career trajectory by fostering their interest in a given specialty, identifying opportunities for early involvement, and facilitating network connections within the field.4,5 Females perceive mentorship to be more valuable to their career development than males, and yet were more likely to report having no mentor.6 Therefore, mentorship of medical students is emerging as a potential strategy for recruiting individuals to certain specialties, but it is unclear if mentees prefer gender-concordant mentorship (i.e., same gender of both mentor and apprentice), and if gender has an effect on the efficacy of mentorship as a specialty recruitment tool.
Improving gender representation among surgeons has never been more important.2 Understanding how inherent career interests, attitudes towards mentorship, and surgical experiences factor into the decision to pursue a surgical career is fundamental to ameliorating student concerns about the specialty and making the surgical environment feel inclusive to all. Accordingly, this study aims to determine if gender differences exist in medical students’ [1] priorities for future practice, [2] mentorship preferences, and [3] surgical clerkship experiences, to ascertain how such differences may affect the decision of female medical students to pursue a surgical specialty.
Methods
Survey Distribution
This cross-sectional study was conducted by surveying medical students at the Oakland University William Beaumont School of Medicine in Rochester, Michigan in April 2020. With Institutional Review Board approval (Protocol #:1575566-1), all grade levels were recruited to complete the anonymous electronic survey via email and social media postings. The survey was created through Qualtrics (Qualtrics XM, Seattle, WA, USA) and made available for one month.
Data Collection
The 18-question survey began with an 8-item questionnaire on demographic characteristics (Appendix A), followed by a set of items inquiring about specialty preferences and motivators, including items related to role models and mentorship (Appendix B). For students who had completed the required third-year surgical clerkship, there was an additional set of 5 questions about the clerkship experience (Appendix C).
Data Analysis
Descriptive statistical analysis was performed in SAS 9.4 (SAS Institute Inc., Cary, NC, USA). Continuously measured variables were compared with Two Sample Independent T-Tests when two groups were being compared and One-Way Analysis of Variance (ANOVA) when more than two groups were being compared. Categorical variables were compared using Chi-Square tests, regardless of the number of groups being compared. Any p-value less than 0.05 (p <0.05) was considered a statistically significant association.
Results
Demographics
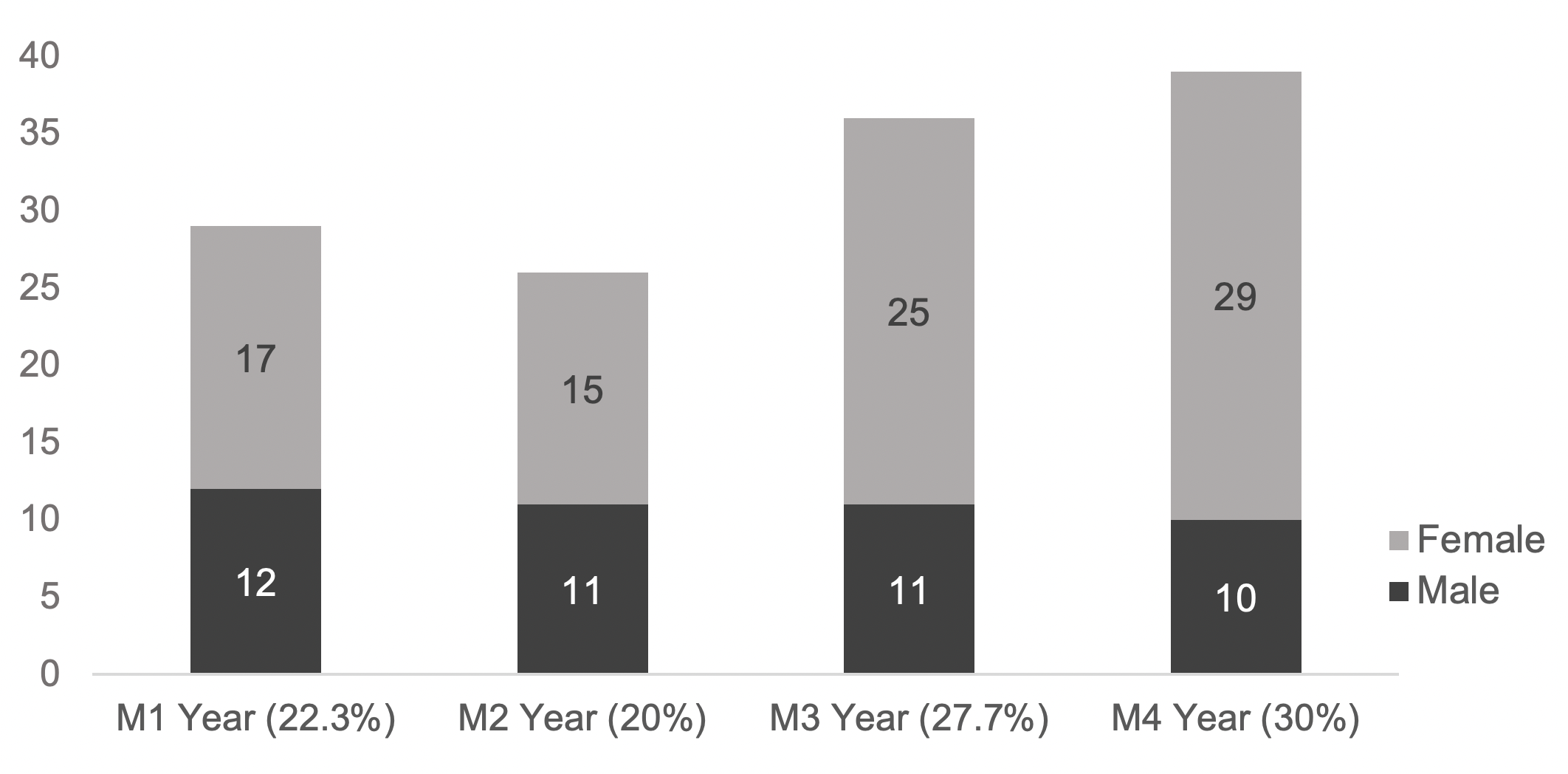
The survey received 131 unique responses, representing 26% of enrolled students. There were 39 (30%) fourth-year respondents, 36 (27.7%) third-year respondents, 26 (20%) second-year respondents, and 29 (22.3%) first-year respondents (Figure 1). Eleven (28.2%) fourth-year respondents had matched into a surgical residency program and 13 (36.1%) third-year respondents indicated plans to apply to a surgical specialty. The majority of respondents identified as female (65.7%). No respondents selected ‘non-binary’ or ‘prefer not to answer’ when disclosing gender identification. Sixty-six (50.4%) of the third- or fourth-year students who responded had completed the required third-year surgical clerkship.

Specialty Interests
Comparative analysis revealed gender differences in specialty interests (Table 1). Female respondents preferred specialties with no surgeries or procedures (p=0.0076) and were less interested in highly specialized practice (p=0.0091), but were more interested in providing preventive care (p=0.0075). In ratings of different factors affecting specialty choice, male respondents placed greater importance on considerations of residency competitiveness (p=0.039) and salary potential (p=0.0205), while female respondents placed greater importance on fears of harassment or discrimination in a given specialty (p=0.0107).
Mentorship Preferences
Female respondents ranked gender-concordant mentorship (p<0.0001) and role models (p<0.0001) as significantly more important to their choice of specialty than male respondents. However, having mentors of any gender was valued more highly than having gender-concordant mentors by both male (p<0.00001) and female (p=0.0041) respondents (Table 2).
Surgical Clerkship
Respondents who had completed the required third-year surgery clerkship were more interested in surgical/procedural practice (p=0.0377), more interested in more specialized fields (p=0.0181), and less interested in providing preventative care (p=0.0152), relative to those who had not completed the clerkship (p=0.0152). Encouragement from instructors, residents, and attendings was ranked as more important to specialty choice among respondents who had completed the surgery clerkship (p=0.0013), while board examination scores were ranked as less important (p=0.0441). Female respondents were less likely to describe the surgical clerkship as “rewarding” (p=0.0212), but there was no significant gender difference in how students rated the surgical clerkship experience (p=0.0894).
Discussion
This study aimed to identify whether gender differences exist in medical students’ specialty interests, mentorship preferences, and surgical clerkship experiences in order to better understand how such differences may influence the decision of female students to pursue a career in surgery. The results suggest a gendered preference for a non-surgical practice among female respondents, despite no gender difference in ratings of the surgical clerkship experience. In other words, the surgery clerkship experience was not perceived less favorably by female respondents even though female respondents reported being less interested in surgery than their male counterparts. Both male and female students valued mentors of any gender as being more important to specialty choice than having gender-concordant mentors specifically. These findings are used to inform recommendations for improving gender representation in surgical specialties.
Reproductive Considerations
Female students were more interested in providing preventive care, less interested in surgical/procedural fields, and less interested in highly specialized practice when compared to male respondents. Female respondents also did not rate salary to be as important in their specialty decision-making as male respondents did. This may be due to inherent differences in the specialty interests of surveyed students, but gender-based considerations may also be contributing. Medical specialties involving more procedures, higher specialization, and higher salary potentials typically require longer training periods which may act as a deterrent for female students.7 While this study did not reveal a statistically significant gender difference in the importance of residency duration on the choice of specialty, it did find a relationship approaching significance between female gender and the ability to start a family during training (p=0.0508), which could indirectly indicate how the required length of training could impact female students’ choice of medical specialty. For the average surgical trainee, delaying childbearing until after residency could mean waiting until their mid to late thirties, which may not be physiologically optimal.8 In order to accommodate for the prospect of childbearing and childrearing during surgical training, residency programs should consider instituting formal parental leave policies and improving the availability of convenient, dedicated lactation spaces and accessible childcare facilities.9
Harassment and Discrimination
Female students prioritized work environment and culture in their specialty selection; valuing a culture that was free from harassment and discrimination. Significant differences were found in the experience of female trainees in male-dominant vs female-dominant specialties, with those in male-dominant fields often reporting more frequent, severe, and stressful micro-aggressive experiences.10 As surgical specialties continue to be male-dominated, female surgeons continue to encounter gender bias. These experiences make female surgeons less likely to recommend their specialty and more likely to leave their field of medicine.10 This may further exacerbate the deterrence of female medical students from pursuing a surgical specialty. Therefore, more needs to be done in order to eliminate harassment and discrimination in surgical environments in order to improve the experience of female surgeons.
Role Models and Mentorship
Gender-concordant role models were more important to the specialty choice of female students than male students. This is consistent with other studies, which have shown that female protégés are more likely to pursue a given career if their preceptor is also female.11 This is also relevant to surgery, where the gender disparity is more pronounced than other specialties and fewer female trainees report having surgical role models.4
Male and female medical students valued mentors of any gender more highly than gender-concordant mentors, indicating that a mentor’s gender was less important than the presence of mentorship itself. This has promising implications for gender-imbalanced specialties. Mentorship is clearly influential in medical students’ specialty choice and may be a useful tactic for recruiting male or female trainees to specialties with fewer gender-concordant role models. For surgical specialties, efforts to establish formal mentoring relationships between surgeons and female students may be an effective strategy to boost interest and promote overall gender equity in the field.
Limitations
Limitations of this study include the small sample size representing a single undergraduate medical education institution. Future iterations of this survey should ensure that questions regarding the curriculum, learning environment, and surgical clerkship experience are applicable to all learning environments, before distributing to other institutions. Respondents were predominantly female (65.65%), which also may have biased the results.
The terminology used in the survey may also present a limitation. Respondents were asked to disclose their gender identity and were presented with the options “male,” “female,” “nonbinary,” or no response. All respondents identified as “male” or “female” and are referred to this way here in this report, however, the terms “male” and “female” describe biological sex and this study was interested in gender differences, not sex differences. These terms were also used in survey questions related to role models and mentors, however, role model and mentor gender and sex were not delineated.
The experiences and perspectives of transgender and nonbinary (TGNB) individuals were not specifically assessed with this survey, but should be addressed in future iterations as research related to the career values and mentorship preferences of TGNB individuals is lacking and should be further studied.12
Conclusions
Gender differences were present in the specialty interests and mentorship preferences of medical students, but not in ratings of the surgical clerkship. This may be due to inherent differences in training and lifestyle priorities, reproductive considerations, and gendered expectations for males and females in medicine. Gender-concordant role models and mentors were more important to female students than male students, which argues for the positive influence of female trainees being able to identify with preceptors in their chosen field. Male and female students valued mentors of any gender more highly than gender-concordant mentors specifically. This has promising implications for specialties looking to improve gender representation; the presence of mentorship is more important to trainees than ensuring gender concordance between mentor and mentee. For surgery, in particular, optimizing gender representation remains an important action item and mentorship of interested trainees may be an effective approach towards accomplishing that goal.
Acknowledgements
We thank Patrick Karabon, biostatistician at the Oakland University William Beaumont School of Medicine, for his help with the statistical analysis of our data.
Funding sources
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.