INTRODUCTION
During the height of the SARS-CoV-2 infection and the associated COVID-19 syndrome in the Northeast, elective surgeries were cancelled as hospitals braced for an onslaught of critically ill patients filling hospital bed capacity. In this time, surgical residents were redeployed to understaffed areas of the hospital caring for COVID-19 patients.1,2 Concurrent with experiencing a substantial adjustment to their residency duties and education, surgical residents also put themselves at risk for infection with COVID-19, often without adequate personal protective equipment (PPE) due to national and hospital shortages.3,4
In addition to the physical risk that healthcare workers faced during this pandemic, difficult triage decisions and high patient mortality have led to moral distress, burnout, and exhaustion.5 In a national survey, the majority of residents respondents reported fearing contracting the disease or transmitting it to their family.4 However, there is a deficit of research describing if surgical residents experienced stigmatization related to COVID-19 by their family or by their communities.
Across the world, there has been harassment of healthcare workers in public places owing to fear of transmission of the virus.6 Our study aimed to determine whether general surgery residents feel stigmatized at work or in public as a result of the COVID-19 pandemic.
METHODS
Survey design and administration
The survey was designed to assess whether general surgery residents feel stigmatized at work or in public during the COVID-19 pandemic. We pilot-tested a questionnaire in a group of 10 general surgery residents to ensure clarity, relevance, and comprehensiveness.
The survey consisted of 23 questions structured as multiple-choice items, open responses, or as statements with a 5-point Likert response scale (Supplement). The anonymous survey was distributed between December 8, 2020 and December 31, 2020 using a web-based tool (SurveyMonkey®) to 172 general surgery residents (both females and males) from 4 academic medical centers in Boston, MA. Subsequent follow-up emails were sent 7 and 14 days after initial query. The survey response tool was set up such that each participant was able to respond only once to the survey. All data were collected in accordance with the requirements of our Institutional Review Board after approval was obtained. Participation was voluntary and responses were confidential. No incentives were offered for survey participation. All data collected are anonymous and participants cannot be identified by residency program.
Data analysis
Only surveys with >80% of questions completed were included in the analysis. Results were calculated based on the number of responses received to each individual question. Open responses were independently coded, and the resulting nominal data are presented as percentage of responses per category. The Mann-Whitney rank sum test was used to compare ordinal scale variables. Statistical significance was set at p<0.05.
RESULTS
A total of 75 general surgery residents completed the survey, corresponding to a survey response rate of 43.6% (75 of 172) over a 3-week collection period. The demographic characteristics of our survey participants are displayed in Table 1.
Approximately 83% (62) of residents reported having interacted with patients infected with COVID-19. The vast majority, 92% (69) of participants underwent COVID-19 testing. While they were required to report the results of their COVID-19 testing to their program leadership, they were more likely to voluntarily disclose the results to their family (4.93/5 on a 5-point Likert response scale), followed by coworkers (4.75/5), friends (4.45/5), mentors (4.20/5), and other relatives (3.91/5).
Among 12 (16%) residents who reported having contracted the COVID-19 infection, 7 of them perceived being judged by their coworkers as being less careful about getting infected outside work. Two of them felt like a burden because their peers had to cover for them while they were on sick leave, and two felt that their peers were uncomfortable being in the same workspace as them despite wearing face masks and practicing social distancing. Outside of work the majority (66.7% [8 of 12]) of residents infected with COVID-19 felt shunned by friends and relatives despite completing the quarantine period.
Seven (58.3%) infected residents reported receiving an overall “good” or “very good” amount of support from their residency program, whereas five (41.7%) of them received “acceptable” support.
Among 73 (97.3%) residents who were aware of a coworker infected with COVID-19, 22 (29.3%) considered their infected peers less careful, assuming they contracted COVID-19 outside of work.
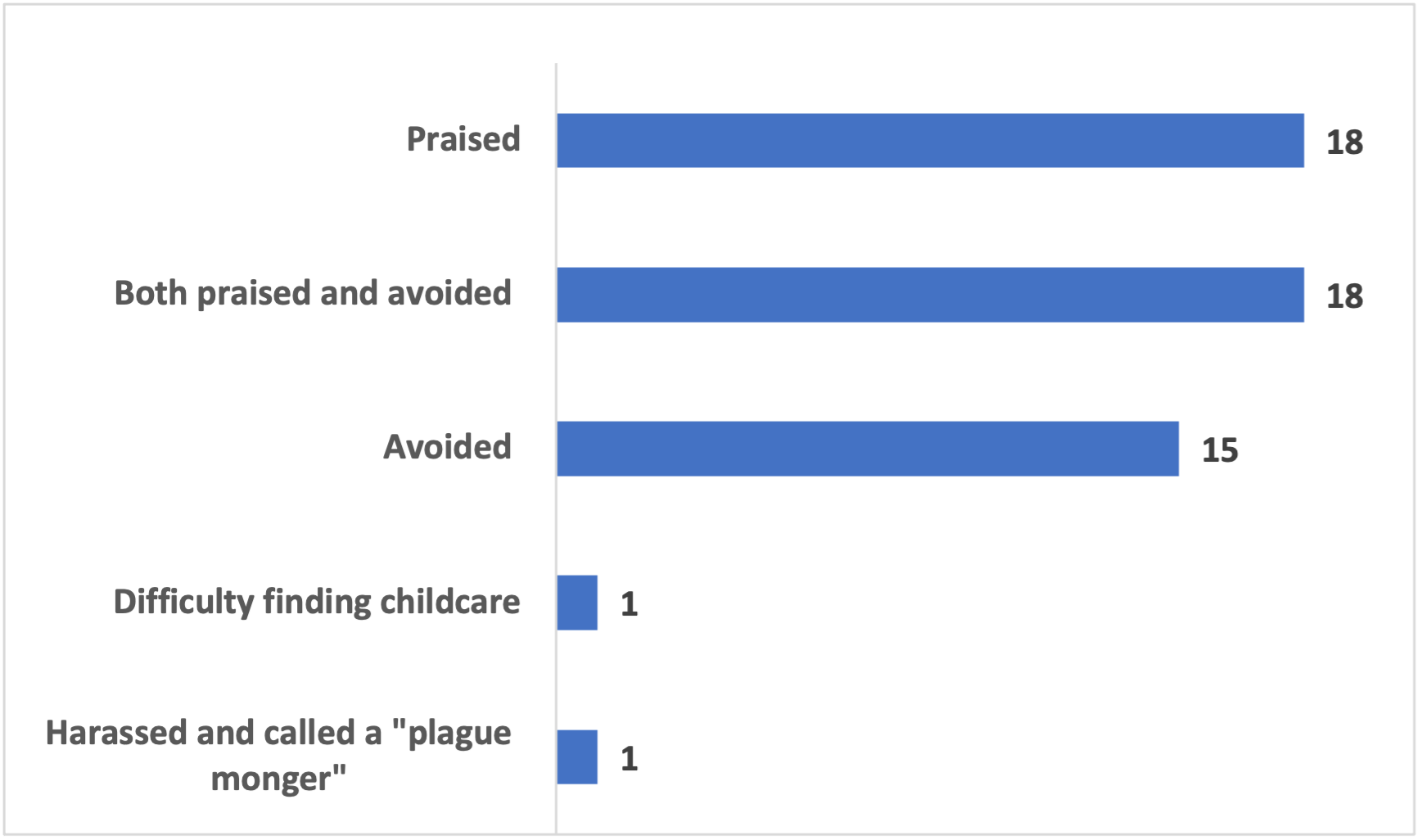
Forty-nine participants (65.3%) felt being treated differently outside of work for being a healthcare worker, ranging from being praised for their work (including receiving tokens of appreciation such as free coffee or moved to the front of the line for groceries) (18) to both praised and avoided (18); avoided despite following universal guidelines (15); having difficulties finding childcare (1); and being harassed and called “plague monger” (1) (Figure 1).

The majority (84% [63 of 75]) of residents who completed the survey are in favor of undergoing routine asymptomatic testing for COVID-19 in the workplace. The reasons for why 12 (16%) residents are against routine testing include lack of clear guidelines about management of asymptomatic residents diagnosed with COVID-19 (6), fear of being stigmatized (4), need to avoid workload issues when residents have to cover for their peers who tested positive (3), and lack of supportive evidence (3).
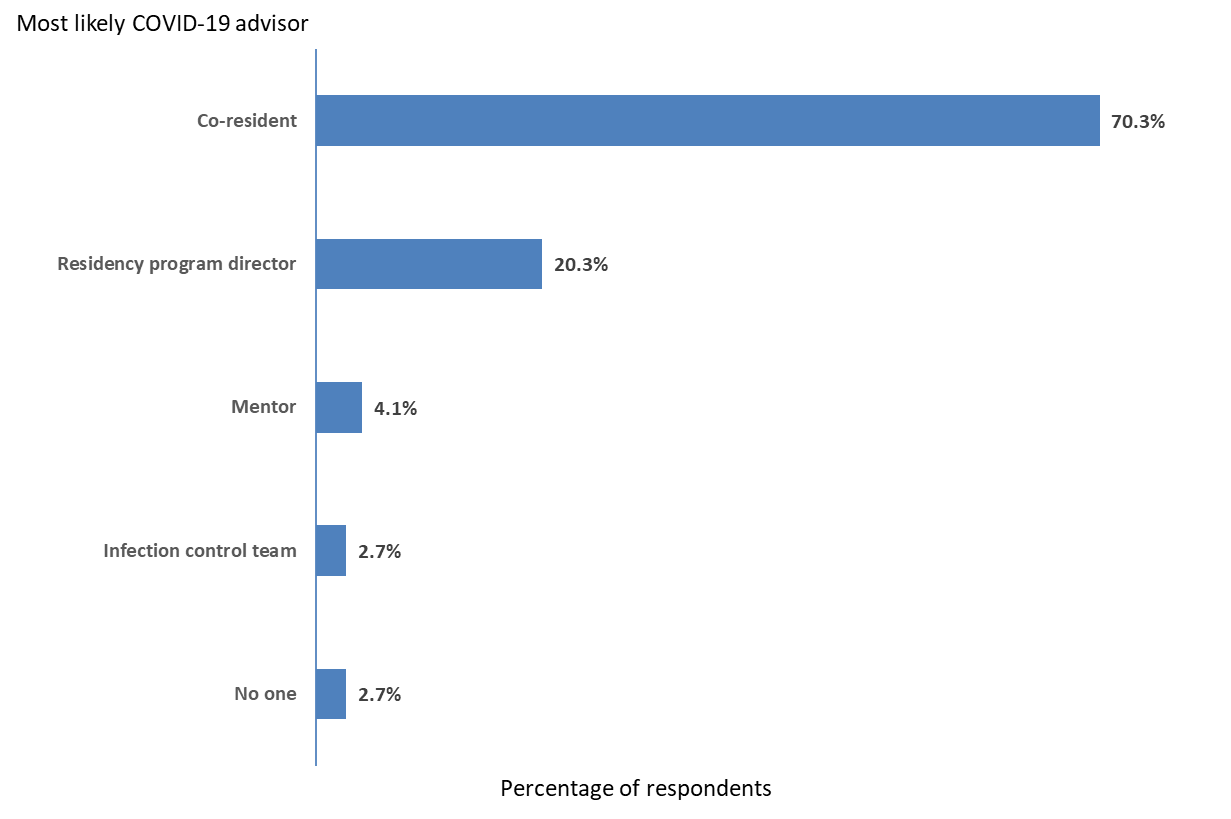
Interestingly, the majority of surveyed residents would feel most comfortable reporting coronavirus-related concerns to their co-residents, followed by their residency program director, mentor, and infection control team (Figure 2).

DISCUSSION
Our multi-center survey of general surgery residents is one of the first to evaluate stigma associated with the COVID-19 pandemic. We found that the majority of study participants felt stigmatized outside of work despite following universal guidelines. In particular, the residents who did contract COVID-19 felt judged and alienated by coworkers. These feelings of stigma are under-recognized and may amplify mental health challenges that are both common in surgical residents and in healthcare providers during the COVID-19 pandemic.
During the pandemic, healthcare workers have received support and recognition as they have faced unprecedented fear, moral distress, and exhaustion.7 The majority of participants in our study report being praised or receiving special treatment for being a healthcare worker. At the same time, many were praised by some and stigmatized by others, which likely reflects the complex socio-emotional environment of the pandemic.8 Being at the receiving end of stigma may increase the challenges of an already demanding surgical residency.9 In a study from Singapore evaluating residents’ experience during the COVID-19 pandemic, it was found that perceived stigma correlated with greater traumatic stress symptoms.10 Furthermore, in a study after the 2003 SARS outbreak, distress persisted among the frontline workers long after the pandemic ended.11 Additionally, resident experience of stigma has potential downstream effects, such as higher rates of attrition, increased burnout, and poorer long-term physical health.12,13
Though the incidence of SARS-CoV-2 infection in residents will reduce dramatically with the widespread administration of the vaccine, it is important to note that over half of the residents who did contract the virus felt judged by their coworkers. This type of behavior harkens back to the HIV crisis, when stigma associated with the virus and the behavioral consequences of stigma permeated healthcare systems across the country.14 At the same time, it is encouraging that our data show that the majority of residents felt comfortable discussing their concerns with some coworkers. Interestingly, only a fifth of residents felt comfortable discussing their COVID-related concerns with their program director. It is possible residents were concerned that their program director would force them to quarantine; this was beyond the scope of the present study. However, this is an area of possible improvement for program directors, as social support, communication, and problem-solving coping mechanisms have been shown to improve stress symptoms in residents during this pandemic.10
The serious complications of COVID-19 have altered the culture of resident sick leave. Prior to the pandemic, there was an ethos of working through illness.15,16 Furthermore, historically, the norms in surgery have equated illness with weakness.17 A survey of residents in New Mexico revealed that many residents avoid or delay medical care because of concern for ostracism by their colleagues and concerns that their peers will have to cover for them.18 Similarly, in our study, residents felt guilty staying home with the understanding that someone would have to take additional responsibilities in their absence. However, coming to work with an active COVID-19 infection can have devastating consequences for patients as well as other healthcare providers and hospital staff. We are called to use this pandemic as an opportunity to ensure that we facilitate a culture shift around illness at work. To this end, we need to guarantee redundancy in programs so that residents can stay home from work without adversely affecting their peers.
The present study has several important limitations. First, our sample size was small, which may limit the generalizability of our results. Second, the participants were limited to a single geographic area and the COVID-19 experience therein. However, our study benefitted from participants at multiple institutions which decreases bias. Third, our response rate was around 50%. There may have been selection bias in those who volunteered to answer the survey and the responses collected may not be representative of all surgical residents. Fourth, our sample size was too small to analyze specific participant demographic characteristics while protecting their privacy. Increased granularity in our data may have provided further insight into subgroups at highest risk of stigma. Fifth, the survey was entirely anonymous, and we were blinded to the respondent’s residency programs. This prevented us from comparing residency programs with regards to the experiences of their residents during the COVID-19 pandemic.
Notwithstanding these important limitations, we hope that our study will increase awareness of the stigma experienced by general surgery residents during the COVID-19 pandemic. Our findings should stimulate further discussions about potential interventions to best support our residents during public health emergencies.
CONCLUSIONS
While general surgery residents are appreciated as essential healthcare workers during the COVID-19 pandemic, they also feel stigmatized despite following universal guidelines. Improving communication about COVID-19 at both societal and institutional levels is critical to supporting the well-being of surgical residents.
FUNDING
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.