Introduction
Epistaxis is one of the most common otolaryngologic emergencies, affecting up to 60.0% of the United States (US) population, with approximately 6.0% requiring medical intervention to control bleeding.1–3 While often self-limiting, severe cases of epistaxis can lead to significant morbidity, highlighting the importance of prompt and effective management. Despite the high prevalence of this condition, previous studies have demonstrated a significant lack of knowledge regarding epistaxis first aid among medical personnel, particularly emergency department physicians.4 Considering its frequency and potential severity, competency in epistaxis management is a fundamental skill for all healthcare providers, including medical students preparing for clinical practice. While prior studies have evaluated epistaxis management among grade schoolteachers and medical students in various regions of Saudi Arabia, corresponding data for medical students in Northern America remain limited.5,6
This study seeks to evaluate the knowledge, confidence, and educational experiences of medical students in North America specifically related to the management of epistaxis. Our work explores potential knowledge gaps, investigates predictors of high knowledge scores, and examines the relationship between self-reported confidence and actual competence. These findings may have implications for medical curriculum development and for improving the preparedness of future physicians to manage this common and potentially life-threatening condition.
Methods
Study design and participants
A cross-sectional study was conducted using an electronic survey distributed to medical students enrolled in accredited medical schools across the US, Canada, and the Caribbean. The survey was disseminated via institutional mailing lists, student listservs, and student networks between January 14, 2024, and January 5, 2025. Participation was voluntary and anonymous, with informed consent obtained electronically before survey initiation. No financial incentives were offered, and only one response per participant was accepted. This study received approval from the Institutional Review Board at the University at Buffalo (Study #00007343).
Survey instrument
The survey consisted of 16 items, including four demographic questions (gender identity, year of study, geographic location, and program type), four education-related questions (prior formal education on epistaxis, clinical exposure to epistaxis, and prior involvement in epistaxis management), and eight epistaxis management questions assessing basic knowledge and clinical decision-making. All knowledge-based questions were in multiple-choice format, covering key domains such as appropriate pressure application, head positioning, duration of nasal compression, prevention strategies, common types of epistaxis, and management techniques for anterior and posterior epistaxis.
Data collection and processing
Survey responses were anonymized, collected electronically via Google Forms, and exported for analysis. Data cleaning involved checking for incomplete submissions and data entry errors. No missing data were identified. For the knowledge-based questions, responses were scored as correct or incorrect based on predetermined answer keys. An overall knowledge score was calculated by summing correct responses across the eight knowledge questions, with a maximum possible score of eight.
Statistical analysis
Descriptive statistics were used to summarize demographic characteristics and survey responses. Continuous variables were reported as means with standard deviations (SD), while categorical variables were presented as frequencies and percentages. Comparative analyses were performed to assess differences between preclinical (i.e., first- [MS1] and second-year [MS2]) and clinical (i.e., third- [MS3] and fourth-year [MS4]) students.
Continuous variables were first assessed for normality (e.g., via the Shapiro-Wilk test). Independent two-sample t-tests were used for variables that were normally distributed, while the Mann-Whitney U test was employed for non-normally distributed data. Statistical significance was defined as a P value < .05. All statistical analyses were performed using IBM SPSS Statistics, version 29 (IBM Corp., Armonk, NY). Logistic regression analysis was conducted to identify predictors of high knowledge scores. High knowledge was defined as a total knowledge score greater than or equal to the median score of the cohort, with students below the median categorized as low knowledge. Variables included clinical year, prior epistaxis management experience, formal education, and self-reported confidence levels. The odds ratio (OR) with a 95% confidence interval (CI) was reported. The correlation between confidence and knowledge scores was assessed using Spearman’s rank correlation coefficient. The overconfidence index was calculated to identify students with high self-reported confidence (≥ 6 out of 7), an arbitrary threshold, but with knowledge scores below the median. Model performance was evaluated using the area under the receiver operating characteristic (ROC) curve (AUC).
Results
Participant demographics and education
A total of 350 medical students completed the survey. Most respondents were enrolled in US medical schools (N = 306, 87.4%). Among these 306 students, 93 (30.4%) attended institutions in the Northeast, 83 (27.1%) in the Midwest, 76 (24.8%) in the Southeast, 46 (15.0%) in the Southwest, and 8 (2.6%) in the West. Respondents’ demographic information is summarized in Table 1. Overall, 255 (72.9%) reported prior involvement in managing epistaxis. In addition, 129 (36.9%) students reported receiving formal education on epistaxis management, whereas 221 (63.1%) indicated they had not received formal training in this area.
Knowledge assessment
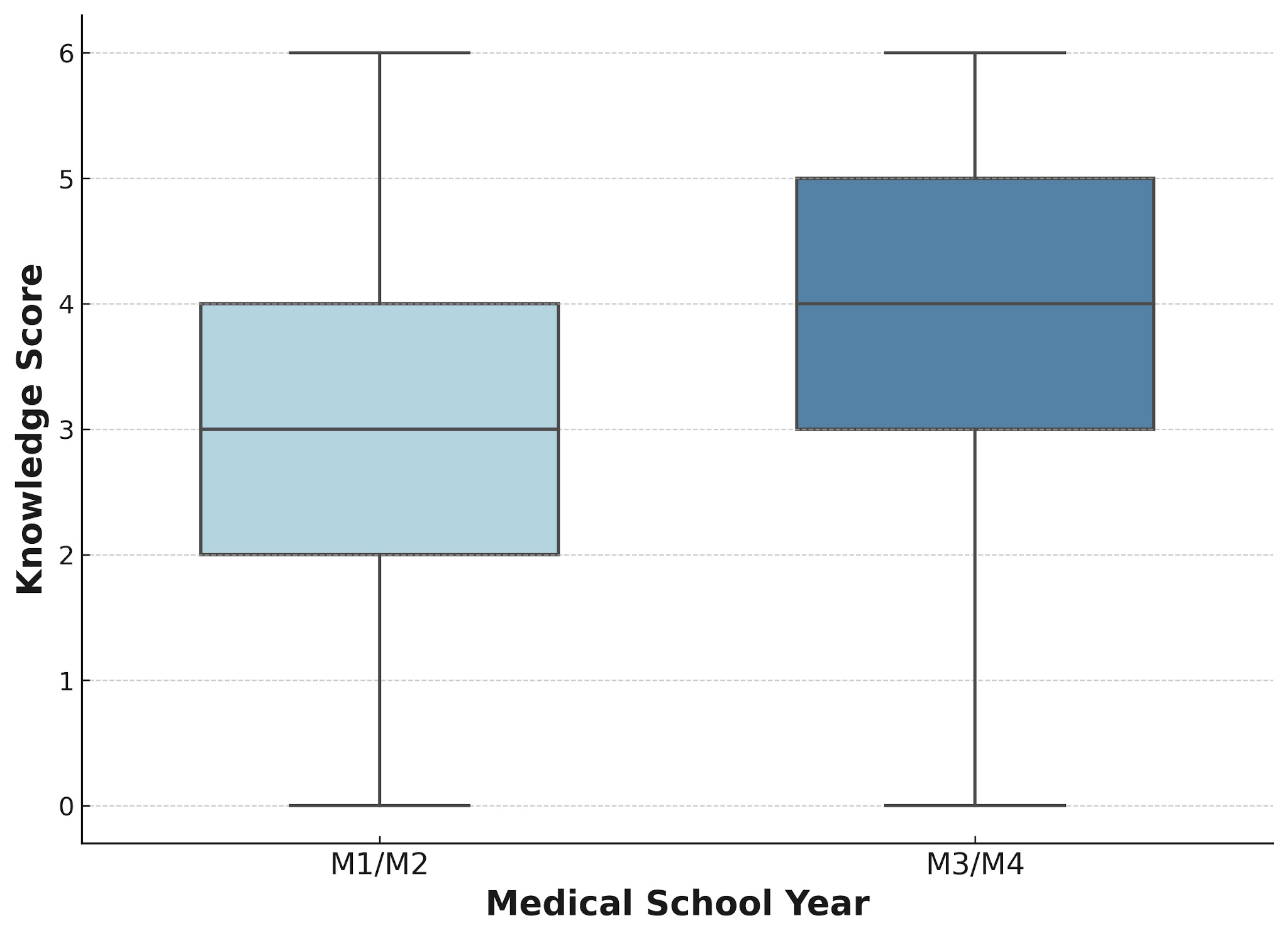
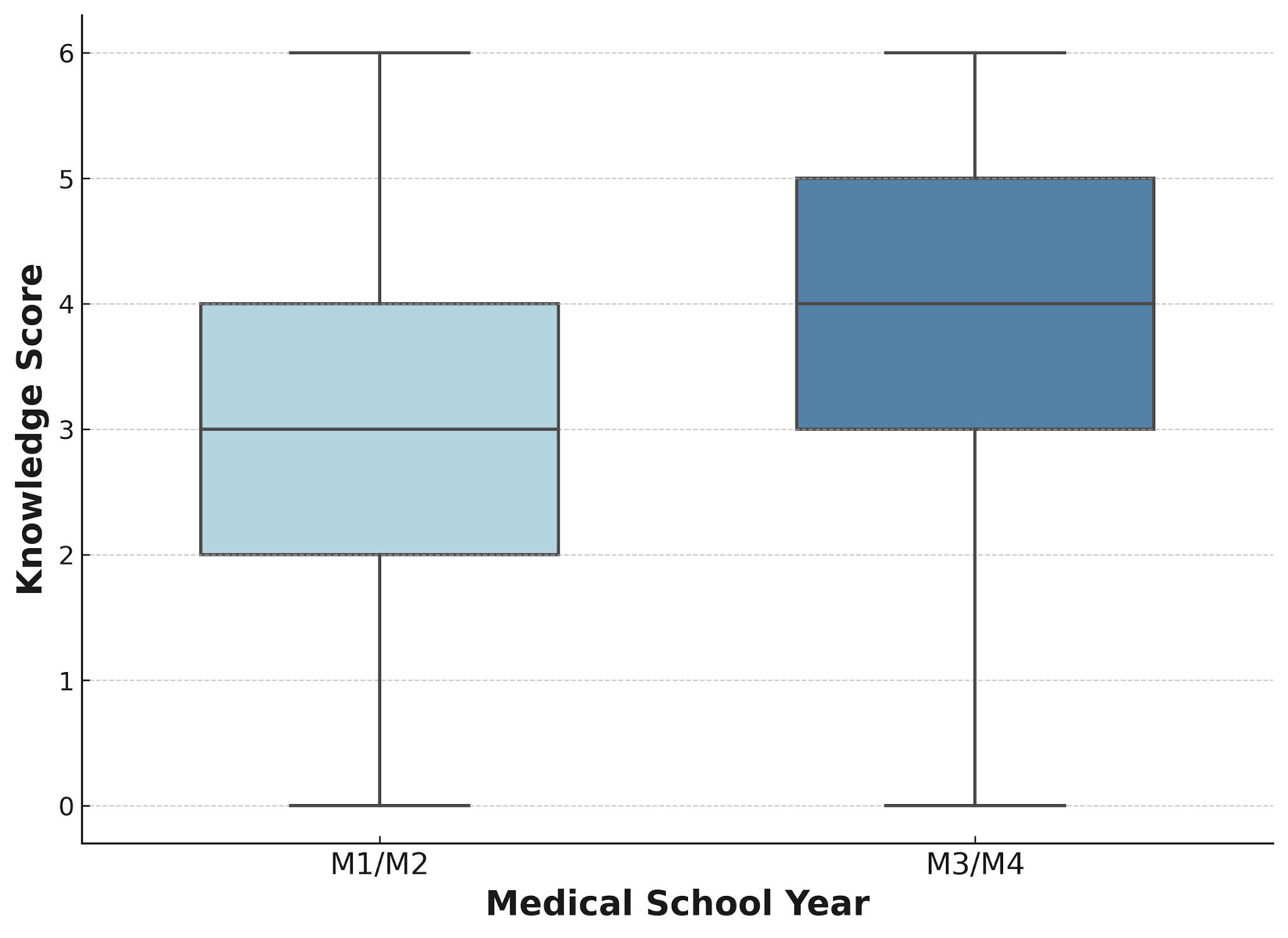
The mean overall knowledge score across all participants was 3.57 (SD = 1.62) out of 8. Clinical students demonstrated a significantly higher median knowledge score compared to preclinical students (4.0 vs. 3.0, Mann-Whitney U = 12,893.0; P = .019; Figure 1). No significant differences in knowledge scores were observed when comparing male and female students (P = .609). Normality testing using the Shapiro-Wilk test confirmed that the data were not normally distributed (P < .001), supporting the use of non-parametric tests.
When comparing specific knowledge items, clinical students significantly outperformed preclinical students on questions related to the preferred head position during epistaxis (N = 110, 72.4% vs. N = 103, 52.0%; P < .001), correct identification of anterior epistaxis as the most common type (N = 114, 75.0% vs. N = 102, 51.5%; P < .001), and knowledge of chemical cautery (N = 106, 69.7% vs. N = 108, 54.5%; P = .004). A summary of response accuracy for epistaxis management questions is provided in Table 2.
Analysis of specific knowledge items identified two critical gaps where less than 50% of respondents provided correct answers. Only 37 students (10.6%) correctly identified the techniques used in the management of anterior nosebleeds, and 31 students (8.9%) correctly identified techniques relevant to posterior nosebleed management.
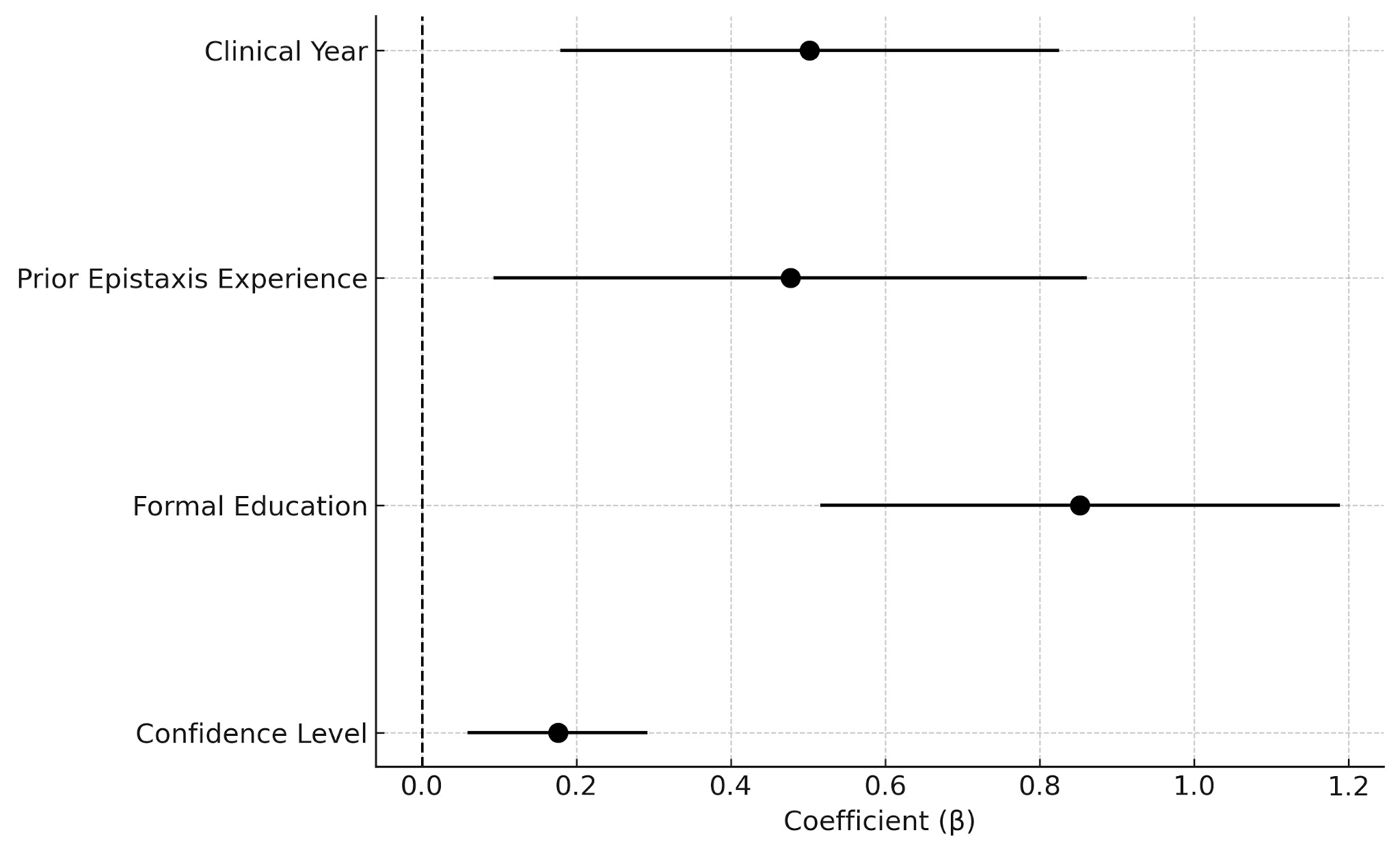
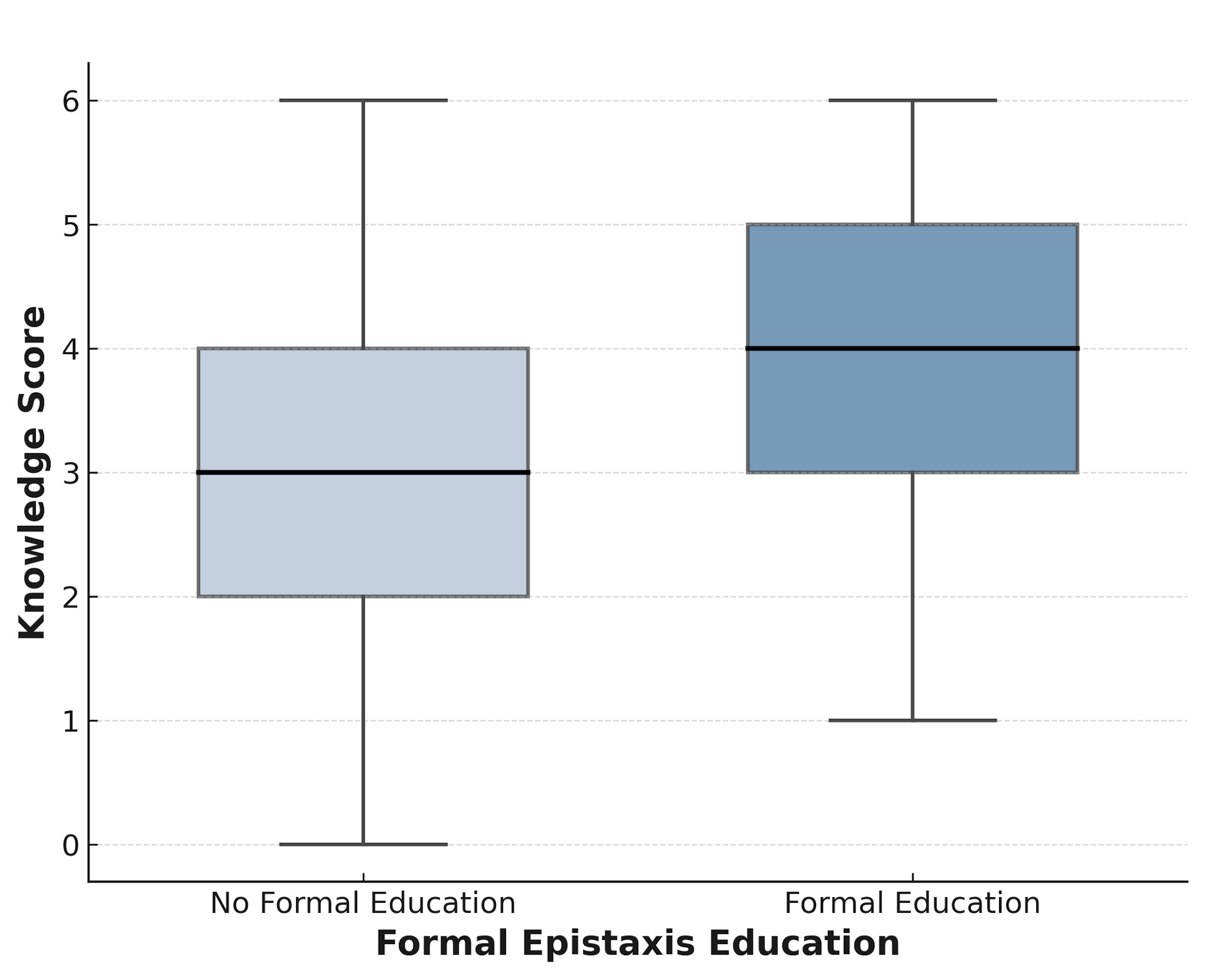
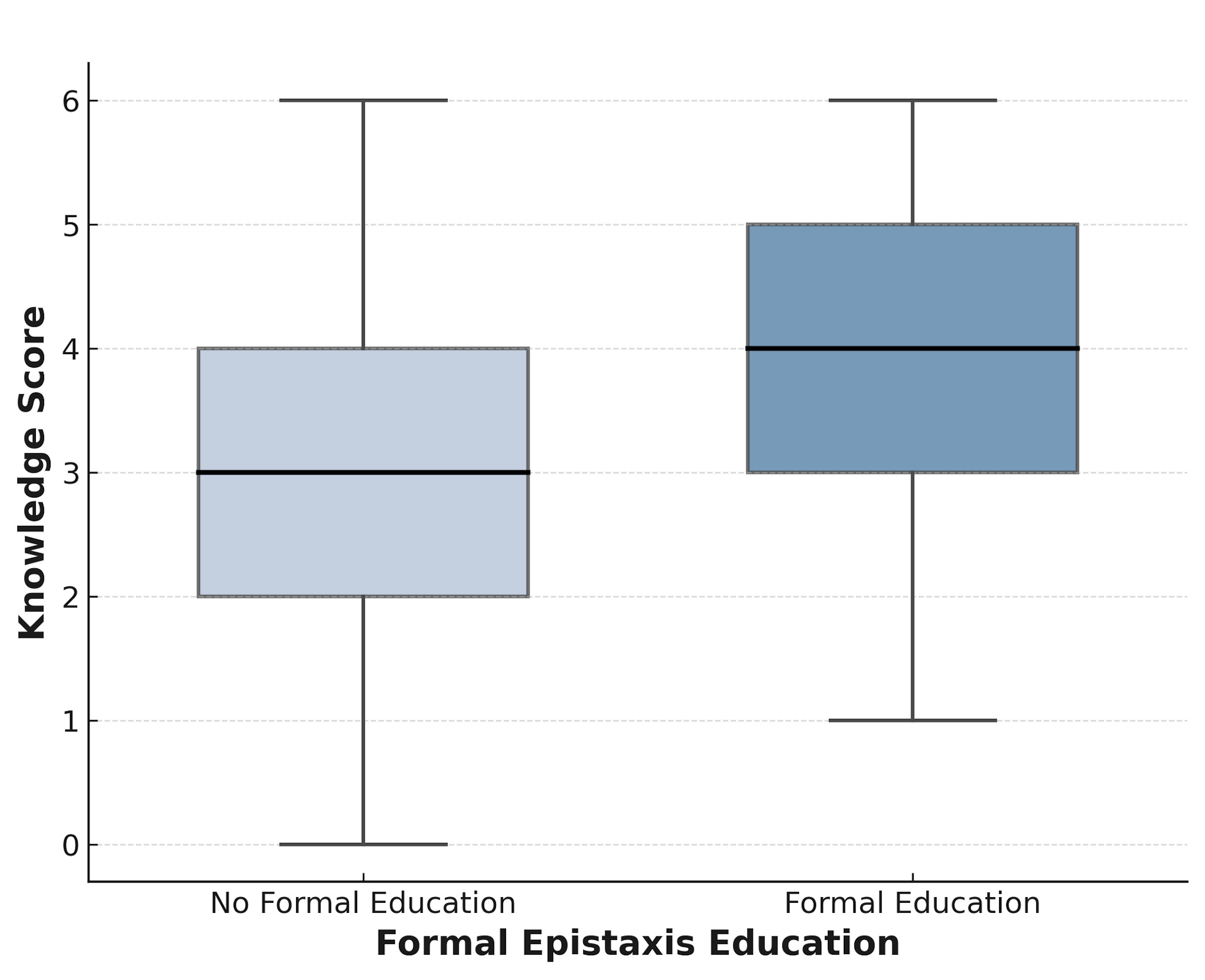
Logistic regression analysis identified formal education (P < .001), clinical year (P = .011), and prior nosebleed management experience (P = .039) as significant predictors of higher knowledge scores. Students with formal education were more than twice as likely to have higher knowledge scores (OR = 2.71). Confidence level did not emerge as a significant predictor (P = .219). Figure 2 provides a visual summary of these associations, displaying the significance of each predictor’s effect on knowledge scores. The impact of formal education on knowledge scores is illustrated in Figure 3, where students who received prior formal education had a significantly higher median knowledge score and fewer low scores than those without (4.0 vs. 3.0, Mann-Whitney U = 8,599.0; P < .001).
_with_95__confidence_intervals_for_predictors_of.png)
Confidence assessment
The median self-reported confidence level in managing nosebleeds was 4. A weak but statistically significant positive correlation was found between confidence levels and knowledge scores (r = 0.28; P < .001). Gender comparisons revealed no significant differences in confidence levels (P = .638). Additionally, no significant differences were observed between Canadian and US students in confidence levels (median = 4; P = .310).
Seventeen students (4.9%) were classified as overconfident, defined as having a high self-reported confidence score (≥ 6 out of 7) while possessing a knowledge score below the cohort median. The confidence calibration curve indicated a slight dip in performance at the highest confidence levels, suggesting potential overconfidence among some students.
Model performance
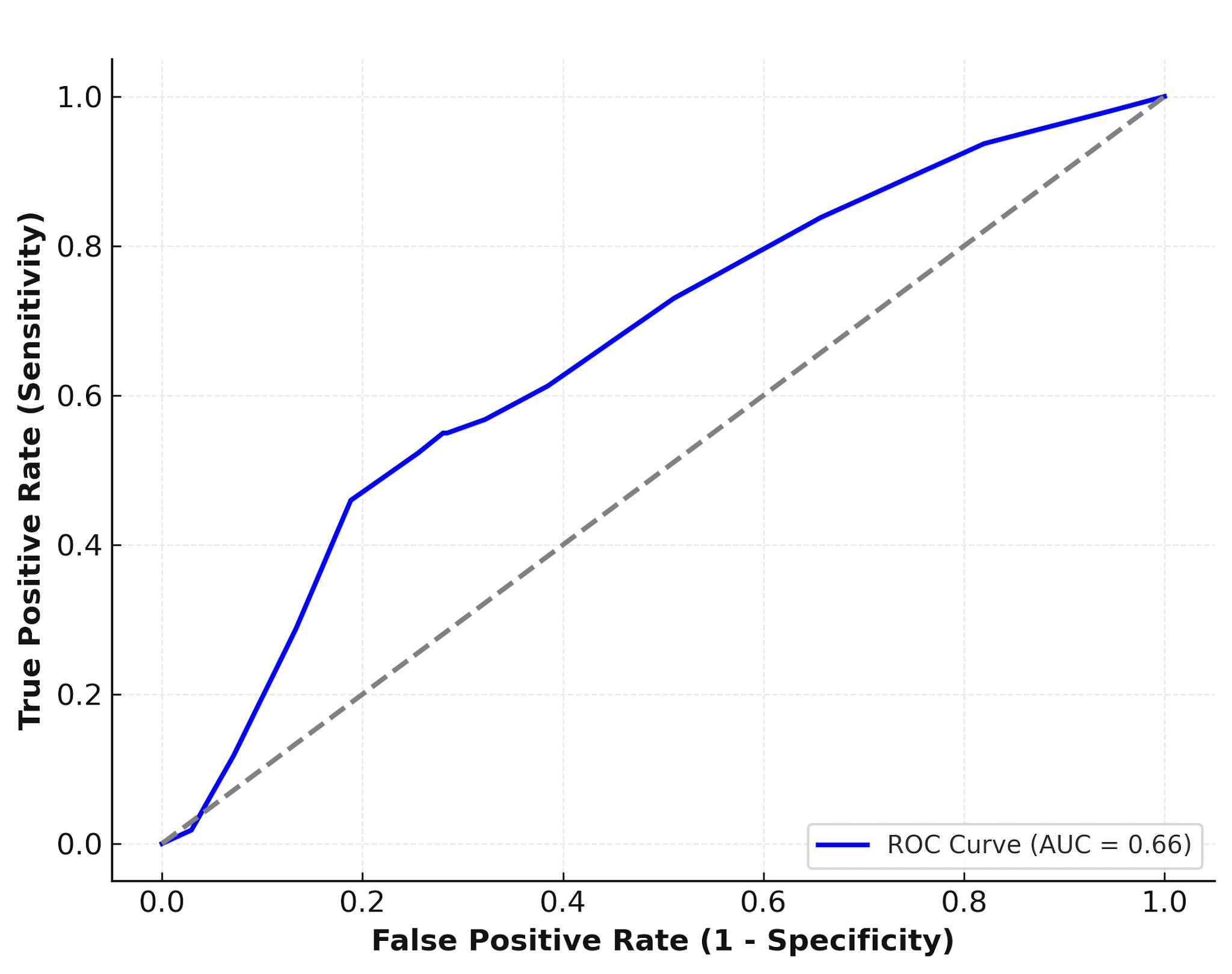
The logistic regression model demonstrated moderate discriminatory capability, as indicated by an AUC of 0.66. The effect size for the difference in knowledge scores between preclinical and clinical students was moderate (Cohen’s d = -0.54). The model’s moderate predictive ability suggests that clinical exposure and formal education significantly contribute to higher knowledge levels in epistaxis management (Figure 4).
_curve_of_the_logistic_regression_model_predicting_.png)
Discussion
This study reveals striking gaps in epistaxis management knowledge among North American medical students across all training levels. With only a moderate effect size between clinical and preclinical students, it is evident that current medical school curricula result in modest, limited improvement in student knowledge of how to competently manage one of the most common otolaryngologic emergencies. These findings raise serious concerns about the effectiveness of medical school education in preparing future physicians to handle acute, real-world emergencies such as epistaxis, which can arise in any clinical setting regardless of specialty.
Two specific knowledge deficiencies identified in this study stood out: (1) only 10.6% of students identified the correct management techniques for anterior epistaxis and (2) only 8.9% of students identified a correct temporizing management technique for posterior epistaxis (e.g., posterior packing), as these are fundamental skills essential for and therefore expected of any frontline healthcare providers. Similar deficits in epistaxis first aid knowledge have been documented across diverse healthcare professionals, including emergency medicine physicians, internists, surgeons, pediatricians, community-based providers, and junior surgical residents.4,7–10 The consistency of findings across both US and Canadian respondents suggests this problem is not confined to one educational system. Rather, it likely reflects a widespread deficiency in how otolaryngology is represented in medical school training throughout North America.
Importantly, this study also highlights the nuanced relationship between knowledge and self-perceived confidence. Although a weak but significant positive correlation (r = 0.28; P < .001), suggesting some level of accurate self-assessment, was observed, further analysis revealed that 4.9% of students were “overconfident,” reporting high confidence despite scoring below the cohort’s median knowledge level. These findings are consistent with prior research. For example, Boldes et al. reported similar miscalibration among junior residents, who universally reported high confidence levels despite demonstration of critical epistaxis knowledge deficiencies, and both Keilin et al. and Kovatch et al. noted that structured educational interventions improved epistaxis management confidence and competence.4,11,12 Conversely, La Monte et al. found that confidence can actually decrease following passive epistaxis management educational exposure such as lectures without simulation, revealing that hands-on practice is essential for meaningful learning.7 Taken together, these results suggest that many medical students are unable to accurately assess their preparedness in regards to epistaxis management, especially when they are not given structured opportunities to develop and apply their knowledge.
Early exposure to otolaryngology has been associated with improved emergency preparedness and greater clinical confidence.13 However, most medical students continue to receive minimal education on even the most essential otolaryngology topics. In the US, fewer than 7.0% of medical schools require a clinical otolaryngology rotation and only 58.9% offer structured preclinical otolaryngology instruction, with Canadian institutions demonstrating similarly limited exposure.14–16 Therefore, one likely contributor to the observed knowledge gaps and confidence miscalibration is the limited integration of otolaryngology into present day medical school education.
Several educational interventions have demonstrated success in improving preparedness for otolaryngologic emergencies, including epistaxis. For example, pilot programs and boot camps designed for both preclinical and clinical medical students have integrated teaching strategies such as simulation-based training, procedural skills workshops, and focused didactic sessions and have shown measurable improvements in confidence and perceived readiness.10,11,17 Similar models have already been implemented effectively in surgical and anesthesiology education, where early, hands-on training is standard practice.10,12 Adapting these approaches for medical student epistaxis management training could serve as a practical and impactful solution to address current gaps in otolaryngology education. By introducing structured, experiential learning into medical school curricula, educators can better ensure that all future physicians are equipped with the skills needed to properly manage epistaxis.
Limitations
There are several limitations of this study that should be considered. First, the cross-sectional design captures knowledge and confidence at a single time point, limiting causal inferences. Second, the survey-based methodology may introduce response biases due to online, self-administration with the potential for students to consult external resources, potentially inflating performance scores. Additionally, convenience sampling through medical student networks may have disproportionately attracted survey respondents with specific interest in otolaryngology, introducing selection bias. If anything, this bias may have led to an overestimation of epistaxis knowledge, suggesting that deficiencies could be even more pronounced in the general medical student population. Finally, the sample predominantly included US medical students, potentially limiting generalizability, although similar trends were observed among Canadian respondents.
Conclusions
This study identified critical deficiencies in North American medical students’ knowledge and confidence regarding epistaxis management. These findings indicate that current educational approaches provide only limited improvement across years of medical school training and may leave students poorly equipped to handle this common emergency. Formal education, simulation-based training, and structured clinical exposure should be integrated into medical school curricula to address these gaps and ensure that all medical school graduates, regardless of their chosen speciality, are prepared to manage epistaxis with both competence and confidence.