INTRODUCTION
Pediatric forearm fractures represent the most common skeletal injury requiring intervention in children, accounting for approximately 25-30% of all pediatric fractures, with an annual incidence peaking at 15.23 per 1000 children in the 10–14-year age range.1,2 While most pediatric distal radius fractures have an excellent prognosis owing to children’s remarkable remodeling capacity, complications do occur, with loss of reduction affecting 7-13% of pediatric forearm fractures overall and rates as high as 62% in older children.3 Importantly, simulation training has demonstrated measurable impact on these outcomes, with orthopedic residents who underwent simulation training achieving significantly less residual angulation (3.7° versus 6.3°, p=0.006), less translation, and lower rates of re-displacement (50% versus 79%, p=0.016) when treating actual patients.4
Despite compelling evidence that simulation-based education significantly improves surgical skill scores, reduces operative time, and enhances learner confidence, skills acquired on simulators have repeatedly been shown to transfer to the operating room; nonetheless, widespread implementation remains challenging.5,6 Cost (89% of participants) and access (76%) represent principal barriers to uptake, with funding barriers negatively correlating with the number of annual simulation sessions.7,8 The most extensively validated simulator for pediatric forearm fracture training incorporates radiopaque bony segments, articulating joints, and simulated periosteum. However, no validated simulators exist specifically for both-bone diaphyseal fractures, and existing models cannot replicate the tactile properties of actual pediatric bone, age-specific remodeling potential, or the clinical judgement required to determine when reduction is necessary.3,9,10 Patient safety concerns further limit opportunities for novice trainees to practice on actual patients, particularly for procedures like pediatric fracture reduction where technical errors can result in re-displacement requiring repeat sedation and manipulation.4
Three-dimensional (3D) printing technology offers potential to address these gaps by enabling production of anatomically accurate, high-fidelity models at substantially lower cost than commercial simulators or cadaveric specimens. The average cost of 3D printing simulators ranges from approximately USD $100-1000, with in-house fabrication demonstrating cost reductions of up to 94.4% compared to commercial models while maintaining comparable educational effectiveness.11–13 Recent advances have demonstrated the feasibility of replicating complex anatomical structures with biomechanical properties comparable to actual bone—polymer lattice structures manufactured via fused filament fabrication can mimic trabecular bone drilling resistance when evaluated by orthopedic surgeons (Likert ratings 2.60-3.00), and optimized resin mixtures can replicate the osteotomy force profiles of human cadaveric bone.14,15 Studies across surgical specialties have shown that 3D-printed models improve fracture classification accuracy, surgical performance, and interobserver agreement compared to didactic learning and traditional imaging, with benefits particularly evident in complex fractures and junior trainees.15–17 Trainee satisfaction with 3D-printed models is overwhelmingly positive, with a combined satisfaction rate of 95% for curriculum integration and 90% for model fidelity.16 However, limitations remain. Poor haptic feedback compared with human tissue is the most frequently mentioned limitation, and some simulators lack integrated structures that allow practice of complete surgical procedures.11,18
The development and rigorous validation of low-cost, high-fidelity 3D printed models specifically for pediatric forearm fracture reduction training could address multiple critical needs: providing accessible simulation training for orthopedic, emergency medicine, and pediatric residents, enabling standardized competency-based assessment, reducing dependence on limited clinical opportunities, and potentially improving patient outcomes through enhanced trainee proficiency before treating actual patients. We aimed to develop and assess high-fidelity, low-cost 3D printed pediatric forearm fracture models and assess their educational utility in teaching novices the principles and techniques of manipulation and reduction in pediatric fractures.
METHODS
Study Design & Participants
Approval was obtained from the school’s institutional review board prior to the start of the study. The workshop was open to all current medical students at our institution’s postgraduate medical school regardless of prior exposure or experience in orthopedic surgery. Participants were invited to complete an anonymous post-workshop survey following completion of the workshop. Participation in the survey was voluntary and had no impact on academic assessment, grades, or participation in future workshops.
Workshop Protocol
The workshop consisted of a didactic lecture followed by a practical session, allowing participants to apply the principles of manipulation and reduction through hands-on practice. The didactic session covered basic fracture biology, pediatric bone physiology, assessment and management of pediatric forearm fractures, and the principles of manipulation and reduction. Following the lecture, students were provided with three forearm fracture models of different configurations – one distal radius fracture, one diaphyseal radial and ulnar shaft fracture, and one proximal third radius/ulna fracture. For each fracture trainer, students were asked to classify the fracture, describe their preferred reduction technique, and practice reducing each model to reinforce how reduction maneuvers are adapted to pediatric bone anatomy and fracture characteristics.
Model Design & Fabrication
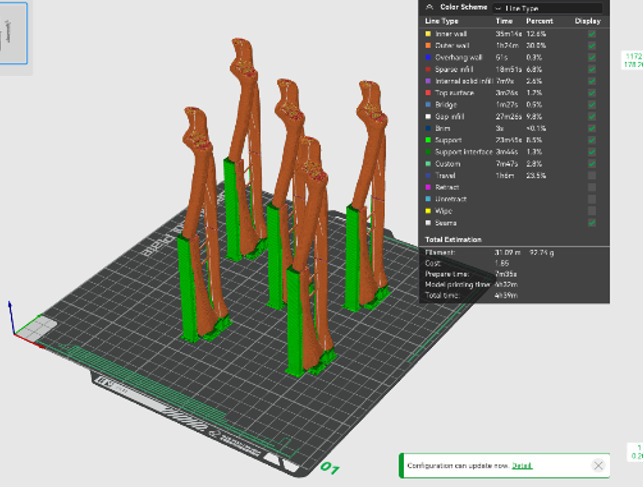
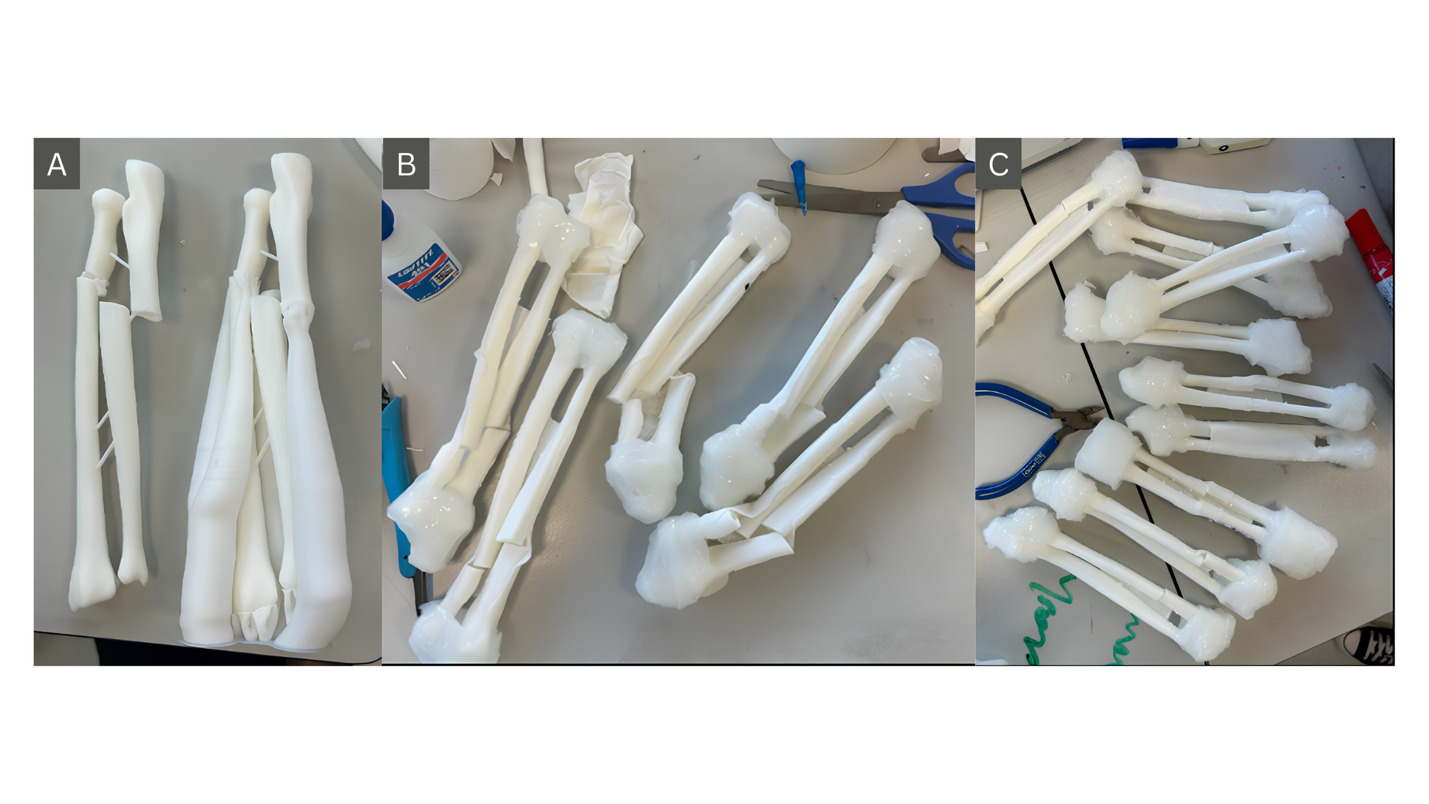
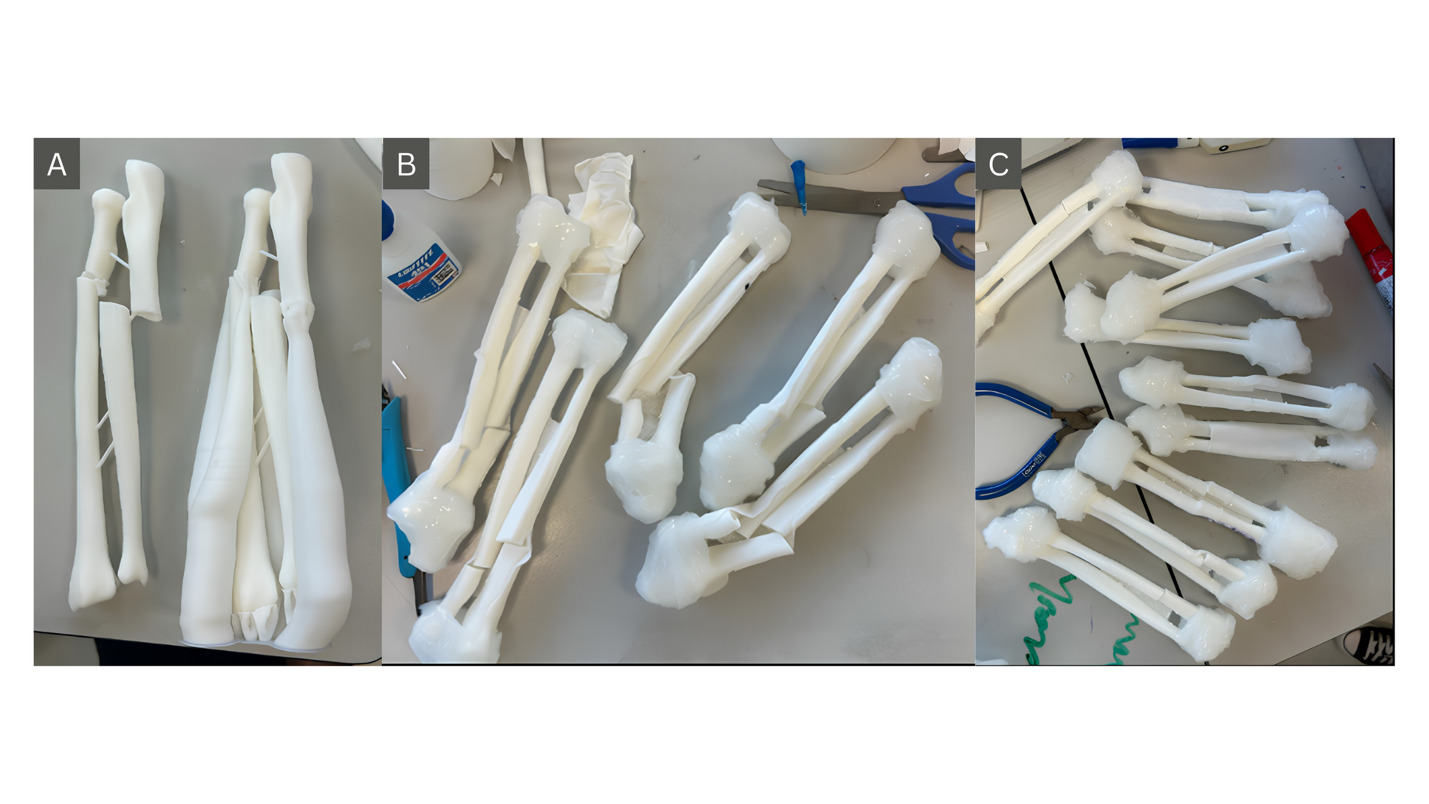
To develop the pediatric forearm fracture trainers, open-source radius and ulna models from Ultimaker Thingiverse were downloaded and resized to pediatric proportions roughly corresponding to the anatomy of a 10-year-old child. The printing medium for bones was polylactic acid (PLA). Following slicing and printing, external supports were removed and clear silicone coating was applied to both ends to simulate the proximal and distal radioulnar joints while maintaining visibility. To simulate the tethering effect of the interosseous membrane of pediatric forearms, stretchable non-woven fabric was stretched between the radial and ulnar shafts and adhered with cyanoacrylate.
Figure 1 demonstrates the digital preparation and slicing workflow, while Figure 2 illustrates assembly of the fracture trainers and the completed models.
_model_for_printing.png)
Outcome Measures
A seven-item Likert scale survey was administered at the conclusion of the workshop to assess participants’ familiarity with pediatric fracture manipulation and reductions, their perceptions of 3D-printed models used in the workshop, and feedback regarding the overall design and pacing of the workshop. Participants were also invited to provide qualitative open-ended feedback. Descriptive statistics, specifically means and standard deviations, were calculated using SPSS Statistics version 29 (IBM Corp., Armonk, NY, USA). The proportion of respondents rating each item ≥4 (agree or strongly agree) was calculated as a summary measure of positive endorsement.
RESULTS
Participant Profile
A total of eleven medical students attended the practical workshop, completed the survey, and were included for in the analysis. Participants ranged from first-year preclinical students to fourth-year students undertaking clinical rotations. Baseline familiarity with pediatric fracture reduction was 2.09 on a 5-point Likert scale. Ten of eleven participants had neither observed nor participated in a pediatric fracture reduction during medical school. A mean score of 1.73 was reported for baseline self-reported ability to perform the procedure.
Educational Outcomes
Following the workshop, mean self-reported familiarity with pediatric forearm fracture reduction increased from 2.09 to 3.91, representing an improvement of 1.82 points. Mean self-reported ability to perform the procedure increased from 1.73 to 3.36, corresponding to an improvement of 1.63 points. Familiarity and procedural ability scores shifted predominantly towards ratings of 4 and 5 following the intervention.
In response to the statement “Having the 3D-printed model helps with my learning”, participants reported a mean score of 4.8, comprising nine ratings of 5 and two ratings of 4. Participants also agreed that the workshop was pitched at the appropriate level and pace for medical students, with a mean score of 4.73 and 100% of the participants giving positive endorsement (rating ≥4).
Table 1 summarizes the survey results.
Cost & Production Analysis
A total of 15 fracture trainers were fabricated for the workshop. In terms of material cost, each bone model incurred SGD $0.87 (USD $0.64) of PLA and SGD $2.69 (USD $1.99) of consumables, including silicone coating, stretchable non-woven fabric cloth, and cyanoacrylate adhesive. The models took approximately 15.5 hours to print, with an additional 11.25 person-hours spent on post-processing and assembly time. This corresponded to approximately three working days for production and preparation. Using an estimated manpower cost of SGD $20 per hour (USD $14.80/hour), the total cost of producing each trainer was SGD $18.56 (USD $13.73).
Table 2 summarizes the resources and costs associated with trainer production.
DISCUSSION
This pilot study demonstrates the feasibility of developing low-cost, high-fidelity 3D-printed pediatric forearm fracture trainers for teaching manipulation and reduction techniques to novice learners. Following a structured workshop incorporating didactic teaching and hands-on simulation, participants reported meaningful improvements in familiarity with pediatric fracture reduction and confidence in performing the procedure. Learner feedback was uniformly positive, with all participants identifying the models as helpful educational tools. Importantly, these outcomes were achieved at a production cost substantially lower than that reported for most commercial orthopedic simulators.11–13
Although self-reported confidence represents a lower-level educational outcome than objective measures of technical performance, it remains a commonly used endpoint in early simulation research, particularly among novice learners. The educational gains observed should be interpreted in the context of participants’ limited prior exposure, with most having never observed or performed a pediatric fracture reduction. The workshop design aligns with principles of experiential learning, whereby learners first acquire conceptual knowledge through didactic instruction before applying and refining procedural skills through deliberate practice in a simulated environment.19,20 By providing a low-risk setting for repeated practice and immediate feedback, the trainers may facilitate progression from cognitive understanding towards procedural competence.21
A notable feature of the trainers was the inclusion of three distinct fracture patterns, encompassing distal radius, mid-shaft both-bone, and proximal-third both-bone forearm fractures. This enabled learners to practice reduction maneuvers while applying fracture classification and treatment planning principles. By integrating clinical reasoning with procedural rehearsal, the models supported a broader educational experience than simple task trainers focused solely on technical execution. Furthermore, the inclusion of both-bone diaphyseal fracture configurations expands upon existing pediatric forearm reduction simulators, which have largely focused on distal radius fracture models.4,9,22
The findings are consistent with the broader literature supporting simulation-based orthopedic education, which has demonstrated improvements in learner confidence, procedural performance, and even patient-related outcomes following fracture reduction simulation training.4,9,23,24 While direct comparison is difficult because of differences in participant populations and simulator designs, our results suggest that affordable 3D-printed models may offer similar educational benefits while improving accessibility. This observation is consistent with systematic reviews demonstrating high learner satisfaction and educational utility of 3D-printed models across surgical specialties.16,17
Cost remains one of the principal barriers to simulation adoption.7,8 Depending on the costing methodology used, each trainer in this study cost approximately SGD $18.56–28.51 (USD $13.73-21.10) to produce, substantially lower than most commercially available orthopedic simulators.11,13 Combined with the use of open-source designs and consumer-grade 3D-printing technology, this may facilitate wider implementation in undergraduate and postgraduate training programs.
Several limitations should be acknowledged. First, this was a single-center pilot study involving only eleven participants, limiting generalizability. Second, outcomes were based exclusively on self-reported measures, and no objective assessment of technical performance was performed. Consequently, the findings are limited to learner reactions and self-perceived confidence gains rather than demonstrated skill acquisition. Third, the absence of a comparator group precludes determination of the incremental educational benefit attributable to the simulator itself beyond the accompanying didactic session. Finally, no assessment of skill retention or transfer to clinical practice was undertaken. In addition, as with many 3D-printed simulators, the biomechanical and haptic properties of the models were not formally validated against human tissue and may not fully replicate the tactile experience encountered in clinical practice.11,18
Future work should incorporate objective performance assessments, evaluation of skill retention and transfer to clinical practice, and formal validation of simulator fidelity. Further refinement of the trainers, including assessment of biomechanical fidelity and radiographic compatibility, may enhance their utility within orthopedic training curricula.
CONCLUSONS
This pilot study demonstrates the feasibility of developing low-cost, high-fidelity 3D-printed pediatric forearm fracture trainers for simulation-based education. The models were associated with improved learner confidence and familiarity with pediatric fracture reduction principles while remaining substantially less expensive than many existing simulation platforms. These findings support the potential role of 3D printing in expanding access to pediatric orthopedic skills training. Further validation using objective measures of technical performance and clinical skill transfer is warranted.