Introduction
Immigration rhetoric in the United States has experienced many changes throughout history. Anti-immigration rhetoric could reduce US attractiveness for highly educated immigrants, because they are more sensitive to the anti-immigration narrative and have greater migration opportunities and more destination choices than less educated immigrants.1,2 Docquier and Vasilakis3 showed that globally, a 10-percentage point increase in the vote share of parties supporting restricting immigration reduces the inflow of highly educated immigrants by 10-percentage point more than those of low skilled migrants.
An important group of highly educated migrants are non-US international medical graduates (IMG). They contribute significantly to the US healthcare system by comprising 25% of the US physician workforce4 Furthermore, compared to US medical graduates, IMGs disproportionally provide care in underserved areas and communities.4–6 Therefore, factors that reduce the IMG participation in US healthcare system, have the potential to negatively impact the physician workforce and healthcare delivery in the United States.
After completing their medical education, IMGs are required to be certified by the Educational Commission for Foreign Medical Graduates (ECFMG) prior to being eligible to apply for residency training and practice in the United States. To become certified by ECFMG, they must pass the United States Medical Licensing Exam® (USMLE) Step 1, Step 2 Clinical Knowledge (CK), and Step 2 Clinical Skills (CS) exams.7 To find a residency training position after obtaining the ECFMG certificate, IMGs, along with graduates of US medical schools, participate in the yearly residency matching process that is managed by the National Resident Matching Program (NRMP).8
Since 1972, the NRMP has published data on the number of non-US IMGs participating in the residency match. In this study, considering participation in the NRMP as one indicator of the overall US attractiveness for non-US IMGs, and we aim to analyze trends in the NRMP published data from 1972 to 2025 to determine whether there is any association with the immigration rhetoric and policies during that period.
Methods
We performed a retrospective cohort analysis of NRMP data generated between 1972 and 2025. Data included the total number of non-US IMGs and US citizens participating in the residency match and their matching rates. We used repeated measures of analysis of variance (ANOVA) to compare differences between time-points of each group. We calculated Chi-Squared test as appropriate to compare categorical data. All statistics were two-tailed, and a p<0.05 was held to represent statistical significance.
We calculated year-over-year (YOY) percent changes in the NRMP participation and matching rates. YOY percent changes of > 15% were considered significant for subsequent time point analysis of possible correlating factors.
For understanding the immigration rhetoric, we conducted a comprehensive review of peer reviewed English literature on immigration published between 1972 and 2025.
For immigration policies we analyzed the immigration legislation passed in the U.S. Congress9 from 1972 to 2025. The Federal Register database10 was used to analyze presidential executive orders on immigration signed from 1972 to 2025.
According to VA Boston Healthcare System policy, our analysis of publicly available data and literature review did not require an Institutional Board Review.
Results
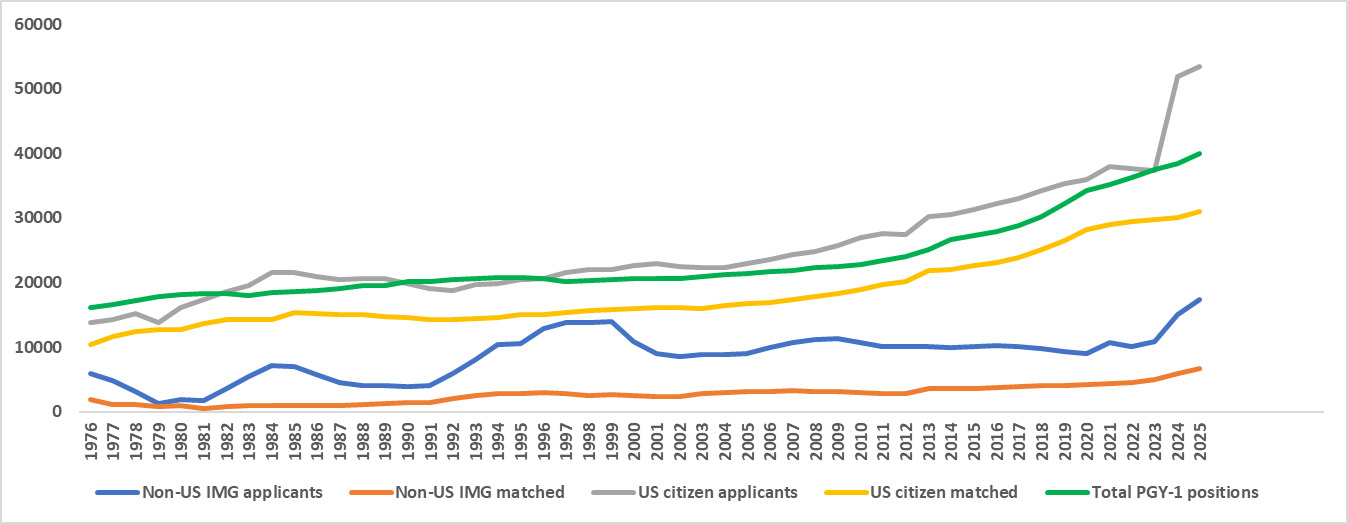
The overall number of PGY-1 positions offered in the match increased from 16,112 in 1976 to an all-time high of 40,041 in 2025 (Figure 1). The number of PGY-1 positions gradually increased through 1994 before declining slowly until 1998. Since that time, the number of PGY-1 positions has only increased.
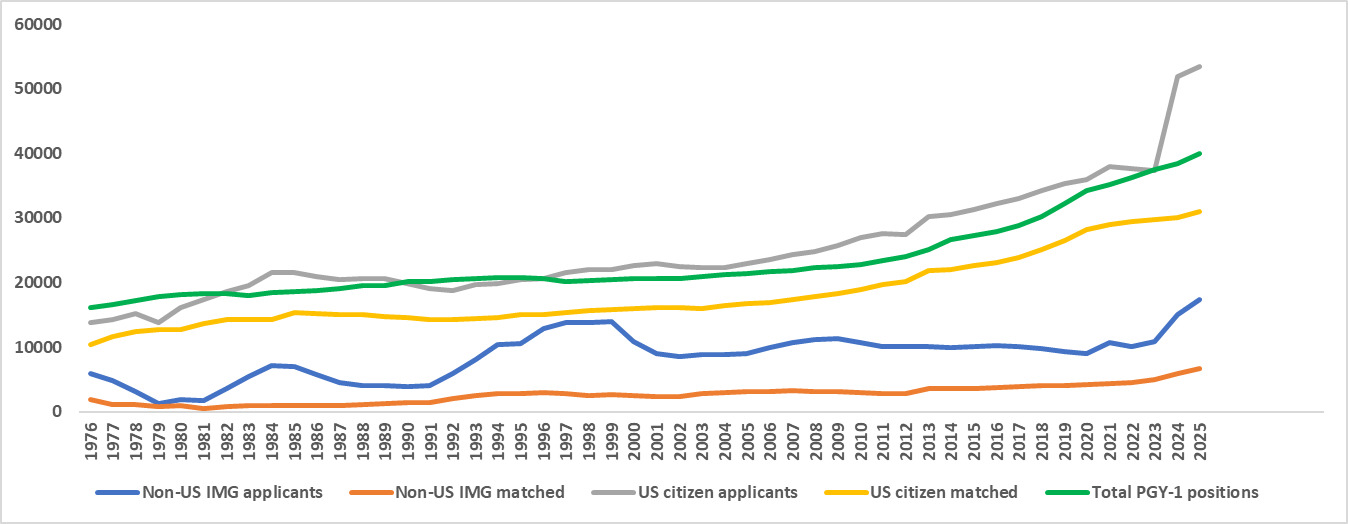
The trend in the number of US citizens applying to the match shows an increase from 13843 in 1976 to 21,511 in 1985. After a decline of 2,709 US-citizen applicants from 1986 to 1992, the number gradually rose each year, reaching an all-time high of 53,503 in 2025 (Figure 1).
The overall number of non-US IMGs applicants has increased from 5,593 in 1976 to an all-time high of 17,382 in 2025. However, the trend in the number of non-US IMGs applicants shows several important fluctuations during this period: decreases during 1976-1979 (4,695 applicants); 1984-1990 (3,208 applicants); 1999-2002 (5,407 applicants); and 2009-2020 (2,309 applicants); as well as increases during 1979-1984 (5,885 applicants); 1990-1999 (10,050 applicants); 2002-2009 (2,689 applicants); and 2020-2025 (8,426 applicants).
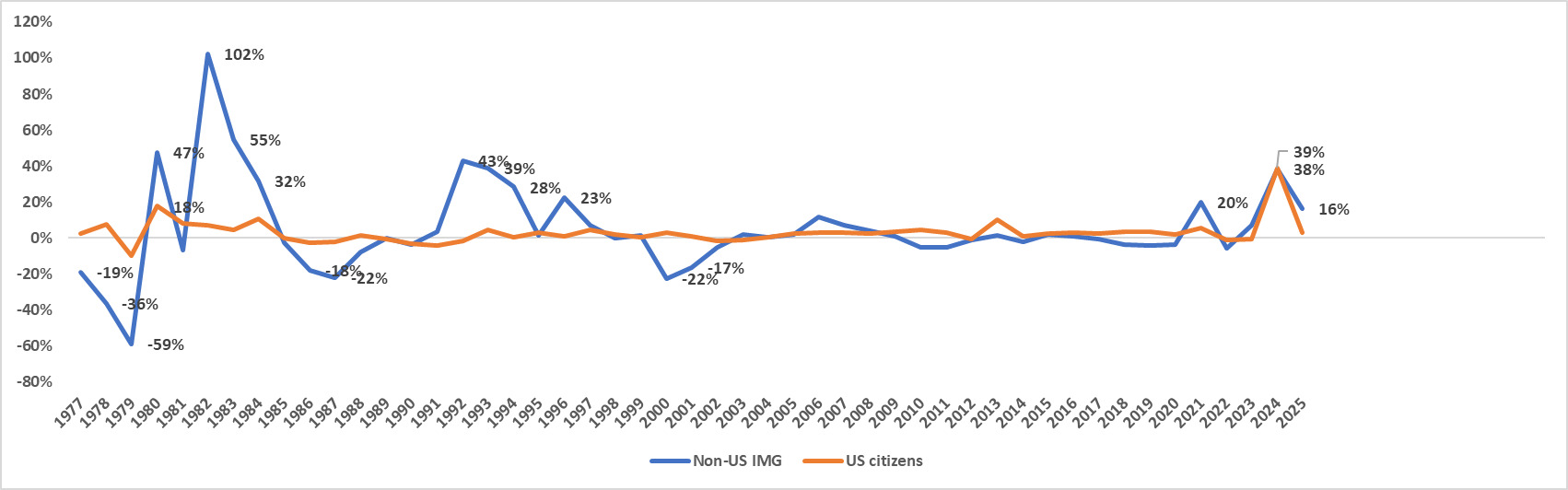
These significant fluctuations are reflected in the YOY percent changes in the number of non-US IMG applicants during the same periods: decreases from -19% to -59% during 1976-1979, -18 to -22% during 1986-1987, -17 to -22% during 2000-2001; as well as increases from +32 to + 102% during 1980-1984; +23 to +43% during 1992-1996; +20% in 2021; +38% in 2024; and +16% in 20205 (Figure 2).
_percent_changes_in_the_number_of_non-us_img_and_us-citizen_applicants.png)
The YOY percent changes in the number of US-citizen match applicants have been stable overall, with only two significant increases, +18 in 1980 and 39% in 2024 (Figure 2).
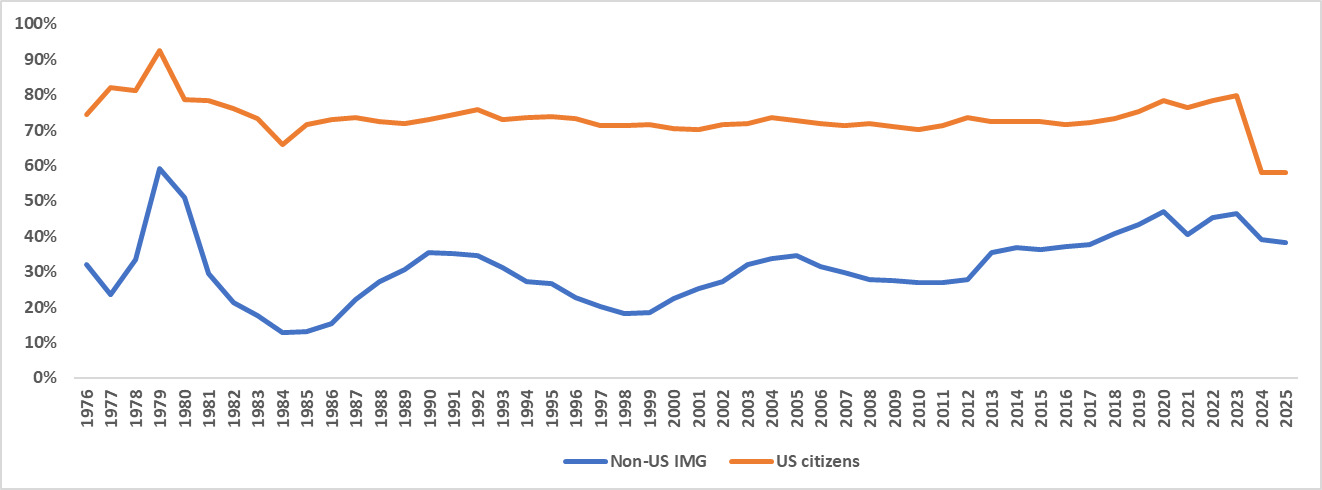
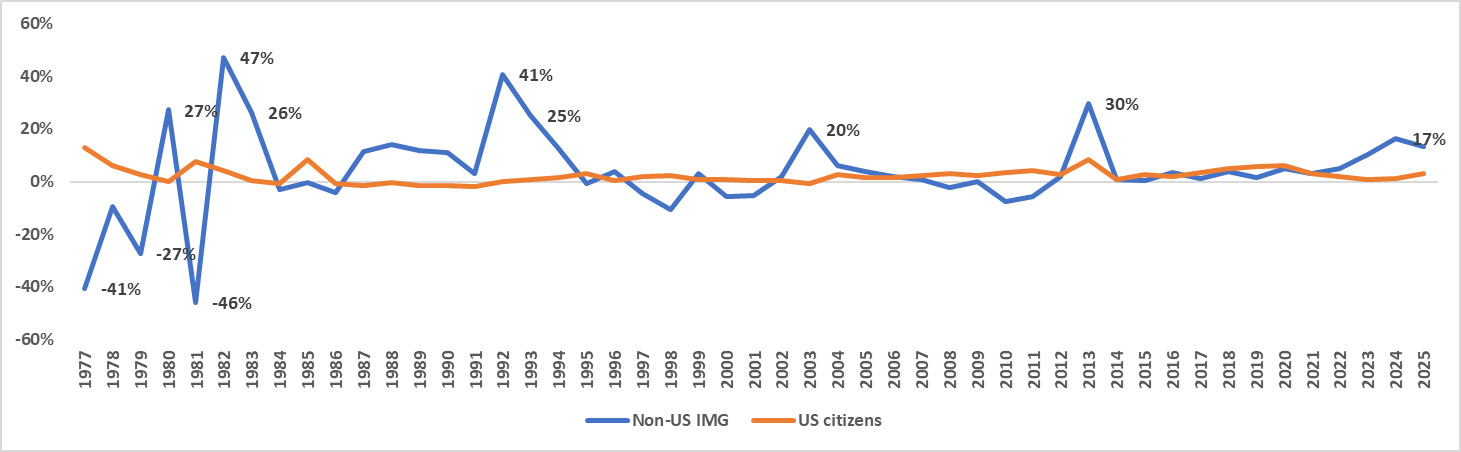
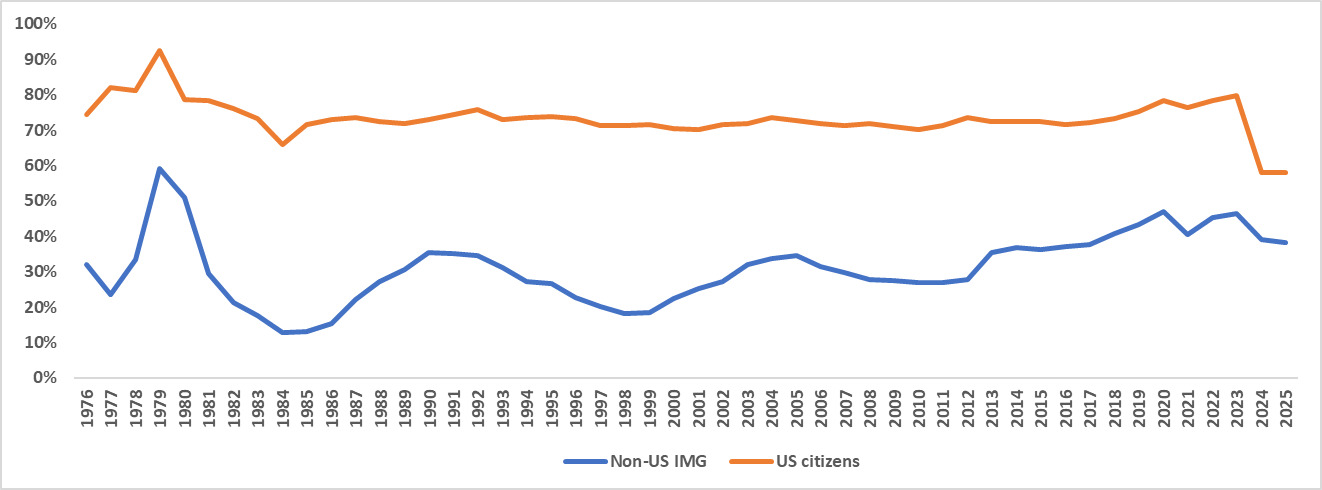
The matching rate of US-citizen applicants from 1976-2025 is 73.6% +/- 4.6% (Mean +/- STDEV), significantly higher than rate of non-US IMG applicants of 31.0% +/- 9.7%. While the matching rates have remained unchanged over years for both groups (Figure 3), only the rates for non-US IMG participants have shown several significant YOY fluctuations: decreases of -41% in 1977, -27% in 1979, -46% in 1981, and increases of +27% in 1980, +43% in 1982, +26% in 1983, +41% in 1992, +25% in 1993, +20% in 2003, +30% in 2013, and +17% in 2024 (Figure 4).
_changes_in_the_matching_rates_of_non-us_img_and_us-citizen_applicants.png)
Our analysis of legislation and presidential executive acts focused on the most important acts that, according to our extensive literature review, have been considered to have had a significant impact on the immigration of IMGs and/or overall immigration to the US. (Table 1).
The Health Manpower Act of 1976
The Health Manpower Act of 197611 was designed to test the adequacy of the medical training that IMGs received in their home countries along with proficiency in the English language. Thus, as a prerequisite for entering the United States IMGs were required to pass an examination equivalent in standard to parts I and II of the National Boards and to be known as the Visa Qualifying Examination (VQE). The number of foreign-born IMG applications significantly decreased after the VQE was established,12 as we demonstrate with decreases of -19% to -59% of IMG applicants from 1976-1979.
The Immigration Act of 1990
The Immigration Act of 199013 was a major overhaul of US immigration laws, signed into law by President George H.W. Bush, that increased the annual cap of legal immigrants, created a lottery system to issue visas to individuals from countries with historically low rates of immigration to the US, created five categories of employment-based visas to admit more skilled workers, increased the family-sponsored visas to help family reunification, revised grounds for deportation, and authorized Temporary Protected Status for individuals from countries with temporary instability.
The Immigration Act facilitated the entry of 20 million people over the next two decades - the largest number recorded in any 20-year period in US history.14 Importantly, the Immigration Act of 1990 significantly increased the number of visas for IMGs, particularly through the H-1B skilled worker visa program. The Act increased the annual employment visa limit from 54,000 to 140,000, which included a higher number of visas for IMGs.13,15 We found a +23 to +43% YOY increase in IMG applicants from 1992-1996 after this went into effect.
Immigration and Nationality Technical Corrections Act of 1994
Typically, a J-1 visa holder (nonimmigrant exchange visitor) is required to leave the United States for two years after finishing the exchange visitor program, including J-1 visa holders who entered the United States to receive graduate medical training. One of the provisions of the Immigration and Nationality Technical Corrections Act of 1994 was the waiving of the two-year foreign country residence requirement for IMGs upon completion of the J-1 exchange visitor program if the physician agrees to practice in an underserved area.16 The institution of this waiving program and subsequent expansions of the cap on J-1 visa waivers significantly increased the supply of IMGs in underserved areas.17
Homeland Security Act of 2002
Following the 9/11 attacks the Homeland Security Act18 instituted more stringent visa application procedures, requiring men from predominantly Muslim countries to pre-register and undergo additional screenings while traveling to and from the United States. Although visa policy itself did not significantly change, the security screening procedures that are part of the visa application process were standardized and intensified after 9/11.19
In addition to safety concerns, the global travel restrictions and economic recession severely curtailed all types of immigration to the US. All these concerns damaged the US image abroad and made it a less attractive destination overall.20
However, the Homeland Security Act did not specifically target international medical graduates and there is no evidence that the temporary decrease in the IMG residency match applications during this period was due to the provisions of the Homeland Security Act, rather as a part of the global immigration decrease after 9/11.
Executive Order 13769, Protecting the Nation from Foreign Terrorist Entry into the US
The Executive Order 1376921 barred for 90 days people from seven predominantly Muslim countries from entering the United States: Iran, Iraq, Libya, Somalia, Sudan, Syria and Yemen.
Because a good number of IMGs practicing in medicine are from the countries affected by the ban,22 legitimate concerns were raised that the order would decrease the number of IMGs from Muslim countries participating in the US residency match.22–24 However, the overall number of IMG’s match participants did not decrease following the travel ban. While it is possible that fewer medical graduates from the affected countries applied after the ban, country-specific data on the match participants are not made available from NRMP to assess a possible correlation.
Political rhetoric on immigration between 1972-2025
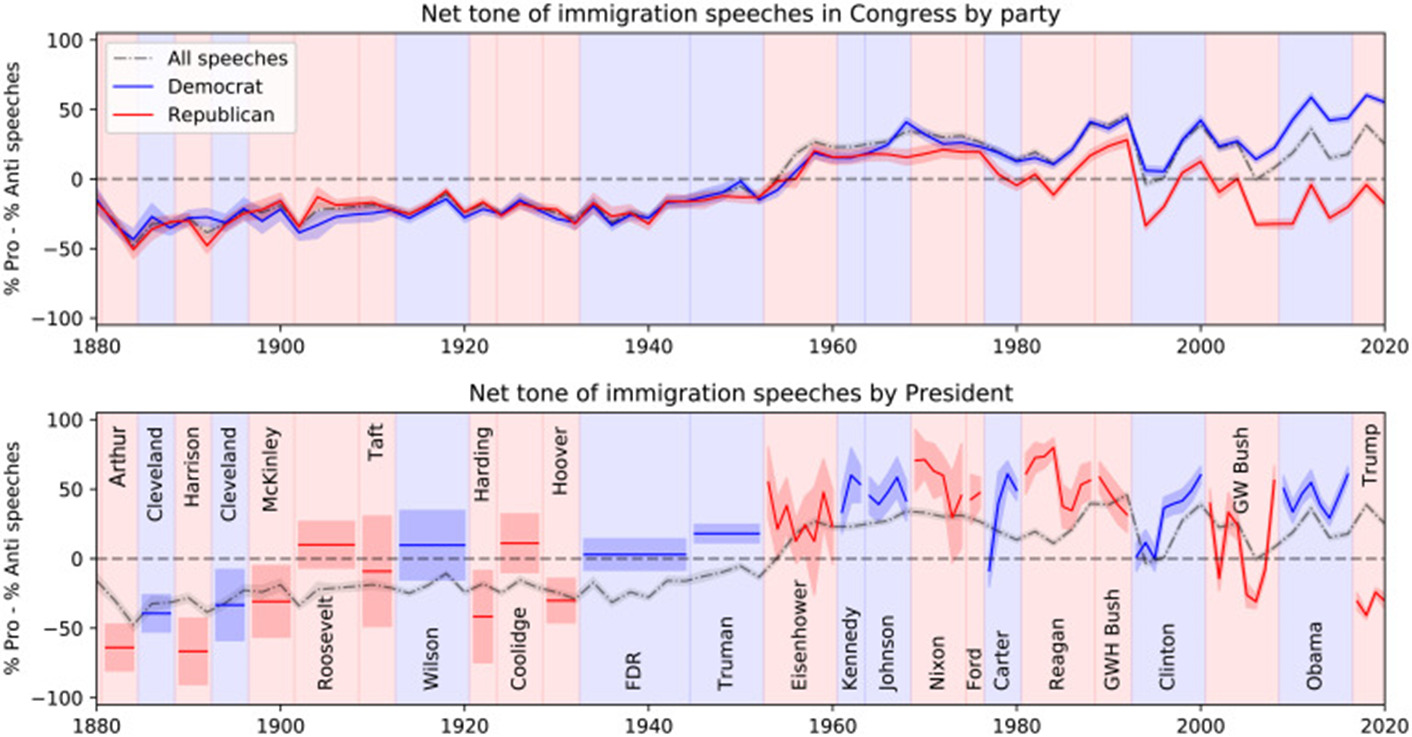
Card et al25 used quantitative text analysis to systematically investigate the language used in 200,000 US congressional and 5,000 presidential speeches related to immigration from 1880 to 2022. Their data shows that both congressional and presidential speeches about immigration have been net positive on average in nearly all sessions of Congress since the early 1950s, and that the overall tone on immigration shifted from negative to positive between World War II and the passage of the 1965 Immigration and Nationality Act (Figure 5). Their analysis also indicates that following the reopening of the border with the 1965 Immigration and Nationality Act, there has been a growing polarization, with Republicans becoming more negative and Democrats more positive on immigrations, with the exception of a transient bipartisan decrease in pro-immigration speeches in the early 1990s, coinciding with the end of the Cold War and the passage of the North American Free Trade Agreement.25
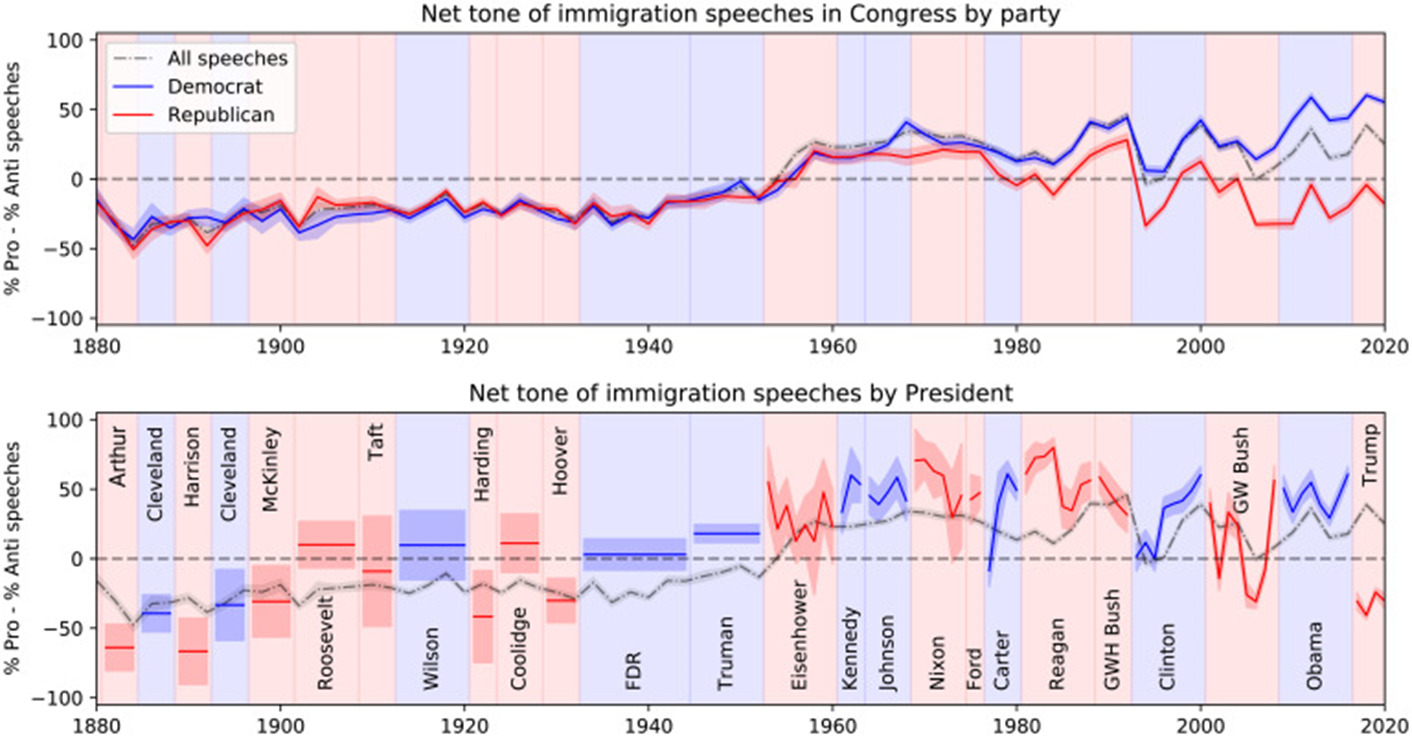
Given the overall net positivity of the congressional and presidential speeches during 1976-2025, politic rhetoric cannot be correlated with the fluctuations in the number of IMGs participants, nor with their matching rates.
Discussion
Immigration policies and legislation have played an important role in shaping the migration patterns and professional opportunities of IMGs seeking to train and practice in the United States. Over the past fifty years, changes in licensing regulations and visa requirements have created both structural barriers and fluctuating pathways for non-US IMGs to enter the US. Our results show that some of these expected fluctuations are directly correlated to legislation specifically addressing immigration of IMGs to the United States, such as the significant decrease in applicants after the Health Manpower Act of 1976 and the subsequent increase after the Immigration Act of 1990.
Surprisingly, our findings do not support a direct correlation between the significant changes in the number of non-US IMGs participating in the match and the political rhetoric on immigration from 1976-2025.
We believe that there are several possible explanations for these unexpected findings. First, the political rhetoric is only one of the many “push” and “pull” factors that influence the attractiveness of the United States for IMGs as manifested by their decision to participate in the US residency match. “Push” factors are reasons that IMGs may have for leaving their home country and are often specific to their country of origin. Some common “push” factors are limited postgraduate training opportunities, under resourced health systems and poor working conditions, political or economic instability, limited career advancement or research opportunities, and social pressures and family considerations.26,27
“Pull” factors are motivations to practice in the United States and include pathways for specialization and fellowship training, structured residency training positions, higher compensation and better working condition, immigration pathways for long term settlement in the US, prestige and global recognition, and higher quality of life for family.27,28
Second, it is possible that the magnitude of the political rhetoric to date may not have been significant enough to tilt the balance between the “push” and “pull” factors in any given direction. Whether the increased magnitude of the negative political rhetoric on immigration of the current administration and its plan institute a $100,000 fee for each H1-B Visa applicant29 will significantly affect the numbers of IMGs participating in the residency match remains to be seen during the upcoming 2025-2026 match.
While immigration policy changes in the United States can have broad implications for our economy, culture, politics, and healthcare, graduate medical education institutions may not always connect these larger policy actions with the complex interplay of “push” and “pull” factors when projecting and planning for our future medical workforce needs. Furthermore, with significant changes in the global political, economic, military, and climate conditions, meeting our current and future physician needs requires a more flexible strategy that is globally coordinated.
It is crucial that our management strategy is ethical and equitable by avoiding the brain drain that is affecting many countries around the world that are losing physicians to immigration to the United States. The WHO Global Code of Practice on the International Recruitment of Health Personnel is a multilevel framework used to tackle this problem, establishing a global model of ethical norms as well as legal and institutional arrangements for recruitment.30 Many low- and medium-income countries already struggle with a low physician-to-population ratio, and when large numbers of newly trained physicians emigrate after training this may exacerbate existing shortages.27,31 This loss can widen disparities in care, especially in rural areas. There is also a loss of public investment in the medical education of these individuals, which is often highly subsidized. This represents a direct financial loss to these countries, as well as the opportunity cost with fewer physicians to serve the local population. As a result, these countries ultimately have slower development of research and academic medicine, further widening the gap, and the remaining staff are at increased risk for burnout given the increased workload.30 The effect of this “brain drain” is complex and a rich subject for further research.
Our analysis has several limitations which should be considered when interpreting the findings. First, our study considers participation in the NRMP as a surrogate for overall US attractiveness for non-US IMGs; however, we could not investigate correlations with their country of origin because country-specific data are not currently reported by the NRMP. As discussed above, there are many country-specific factors which contribute to emigration at a political, economic, and social level. It is therefore impossible to analyze possible correlations with legislative and executive acts targeting immigration from specific countries, or to correlate with many “push” factors. Second, because the 2026 NRMP match results will become available on March 20, 2026, this study does not analyze the impact on IMG match participation of the recent and dramatic changes in political rhetoric and policies since the start of the new administration on January 29, 2025.
Third, several large changes in ECFMG certification requirements and USMLE examination structure might have further affected IMG participation in the residency match. For example, the 1998 introduction of the ECFMG Clinical Skills Assessment (CSA) and its 2004 replacement by USMLE Step 2 CS added financial and logistical barriers for IMGs, potentially lowering participation in the near term.32 More recently, the permanent elimination of Step 2 CS in 2021, the transition of Step 1 to pass/fail scoring in 2022, and the implementation of the ECFMG 2024 Accreditation Requirement-which requires IMGs to graduate from a medical school accredited by an agency recognized by the World Federation for Medical Education-have changed the incentives and pathways to U.S. training for IMGs.33 Such regulatory changes can affect IMG application behaviors independently of immigration rhetoric or legislation, and their cumulative effect may partially account for year-to-year variations in NRMP participation.
Notwithstanding these limitations, our study highlights the importance of our graduate medical education organizations understanding all the factors that can influence IMGs’ participation in our healthcare system.
Conclusions
While immigration political rhetoric alone does not influence the non-US IMGs plans of participating in the US residency match, immigration policies specifically addressing IMGs can have a direct impact. Graduate medical education organizations should consider all factors that could affect the US attractiveness for non-US IMGs to adequately meet our physician workforce needs and avoid doing so at the expense of other countries.
Author contributions
Racel Huselid: Writing- Original draft preparation, Writing- Reviewing and Editing. Mario O’Connor: Writing- Reviewing and Editing. Patrick Soonthornprapuet: Writing- Reviewing and Editing. Edward Whang: Writing- Reviewing and Editing. Gentian Kristo: Conceptualization, Methodology, Formal analysis, Writing- Original draft preparation, Writing- Reviewing and Editing, Supervision.
Disclosure statement
The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article.