Introduction
In 2013, the President of the World Bank challenged the first Lancet Commission on Global Surgery to establish surgical care as a cornerstone of global health.1 Since then, significant progress has been made in advancing global surgical initiatives, accompanied by growing interest in international outreach.2,3 Urologists have actively followed this trend, contributing to the expansion of surgical care worldwide.4 Global surgery initiatives aim to expand access to safe, timely, and affordable surgical care in low- and middle-income countries (LMICs). Within urology, these efforts often address a broad burden of disease, including trauma, malignancies, and congenital anomalies.5 Procedures performed range from reconstructive surgeries to endourologic interventions, typically targeting service gaps in host communities.
While enthusiasm for global surgery grows, designing ethical, sustainable, and impactful programs remains a challenge. Effective initiatives must align with both local healthcare needs and institutional priorities, emphasizing long-term partnership, education, and surgical capacity-building over episodic mission-based care.
Additionally, the appropriate role of U.S.-based trainees in global surgery initiatives remains a source of debate.6,7 While trainees may express interest in global health, some urologists are concerned that their involvement may disrupt local training or divert resources away from sustainable development goals of training local surgeons.8
Despite these priorities, there has been little systematic investigation into the perceptions of academic urologists regarding various forms of global engagement—including direct patient care, teaching, virtual education, and support for research. The purpose of this study is to evaluate the scope of participation in global urology initiatives among academic urologists and to assess their attitudes about global engagement, including perceptions of its clinical and educational impact, institutional support, and the value and appropriateness of trainee involvement. These findings aim to inform the design of future initiatives and promote policies that support ethical, collaborative, and durable global surgery programs.
Methods
This study was a cross-sectional survey of academic urologists to assess experiences and attitudes related to global surgery (Supplemental Material). The survey was distributed electronically via the Society of Academic Urologists (SAU) email listserv, residency program administrators, and the Society of Genitourinary Reconstructive Surgeons. Duplicate responses were excluded based on self-report of prior completion.
Eligible participants included urologists affiliated with academic institutions, including faculty with clinical, educational, or leadership responsibilities.
The survey instrument included questions on:
-
Demographics (age group, gender, fellowship training, years in practice)
-
Professional roles (e.g., program director, department chair, faculty)
-
Experience with global urology work (number of trips, funding sources, type of involvement)
-
Perceived impact of prior global work on patient care and training of local providers
-
Attitudes toward institutional support, academic credit, and time allocation for global volunteer work
-
Interest in future participation (e.g., operating abroad, teaching, virtual education)
The survey utilized a mix of categorical, Likert-scale, and open-ended questions.
Descriptive statistics were used to summarize respondent characteristics, global surgery experience, and attitudes. T-tests and logistic regressions were used to analyze results. Analyses were conducted using Stata 18.5 (StataCorp LLC, College Station, TX).
Results
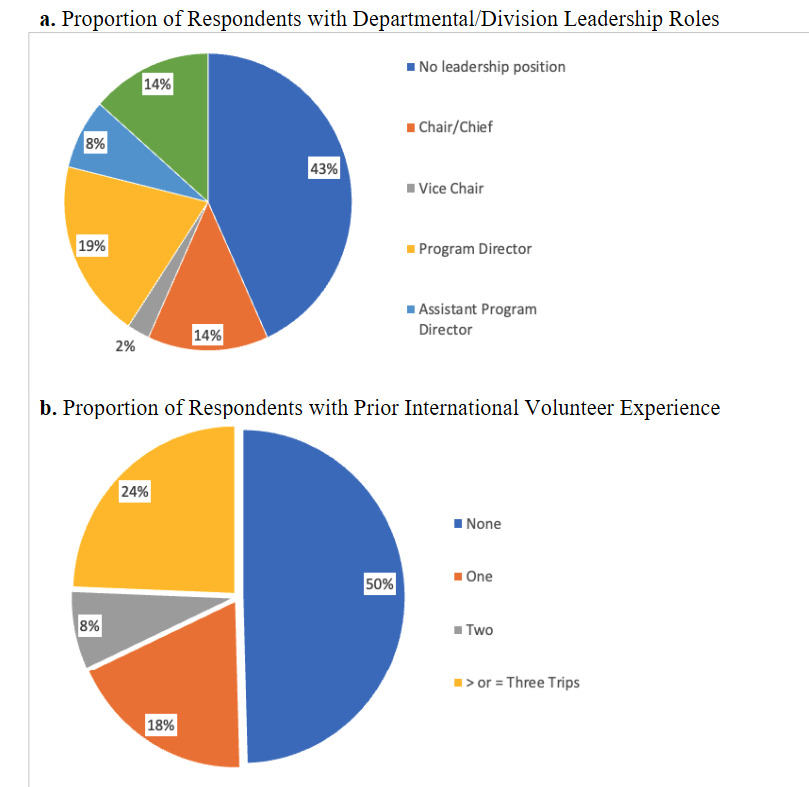
A total of 119 urologists completed the survey. Table 1 displays cohort characteristics of the respondents. The majority of respondents (95%) were affiliated with academic programs. Most respondents were male (70%), and 80% reported having completed fellowship training. The median number of years in practice was 10 (IQR: 5–21). Leadership roles were common: 16 respondents identified as department chairs, 3 as vice-chairs, 23 as program directors, and 9 as assistant program directors, collectively comprising 43% of the sample (Figure 1a).
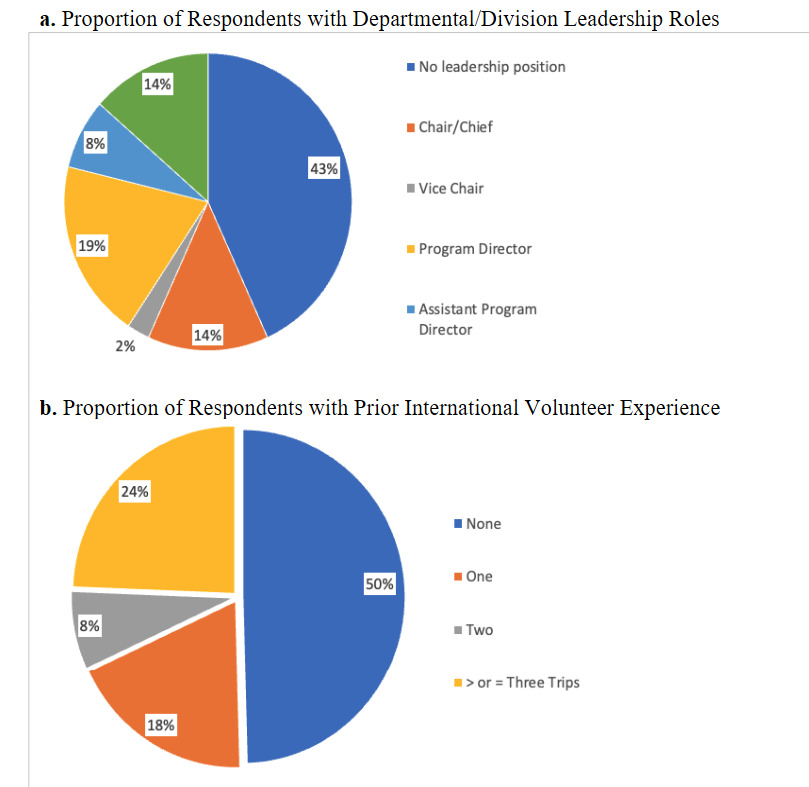
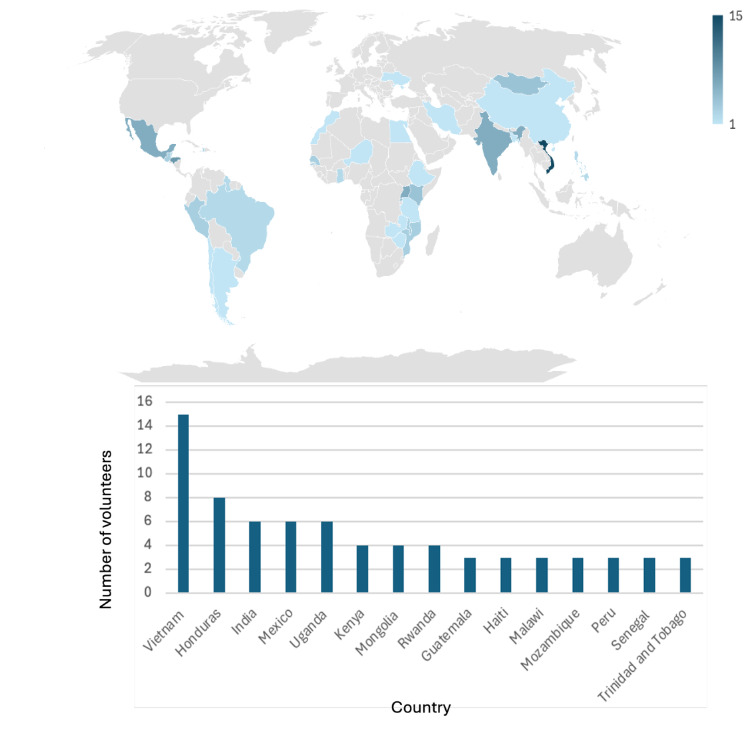
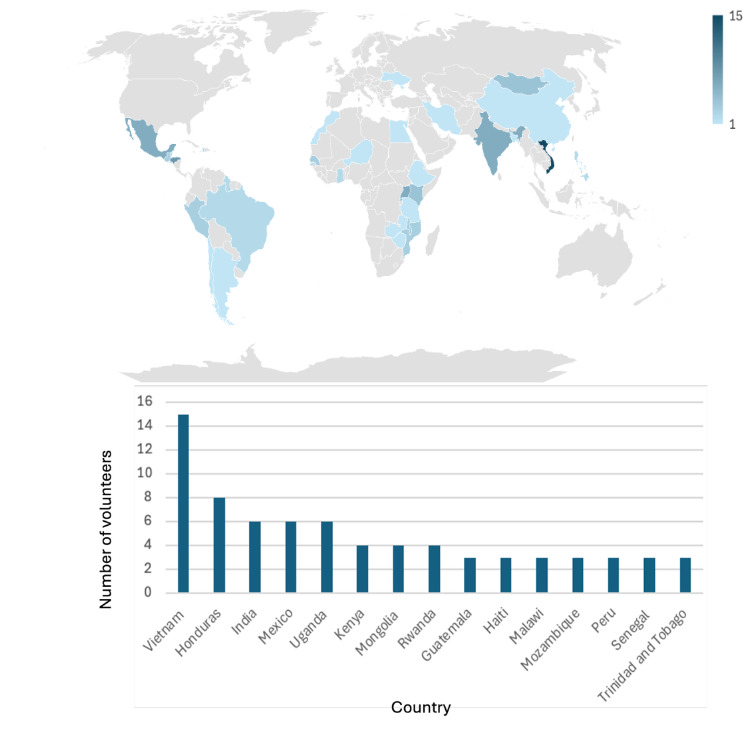
Regarding global health participation, 50% of respondents had engaged in at least one global urology experience, while 32% had participated in multiple (Figure 1b). Participants had volunteered in 38 countries across 5 continents (Figure 2). Among those with prior experience, 68% had self-funded their travel at least in part, and 55% reported receiving some form of departmental or organizational financial support. However, only 51% of all respondents were aware of institutional funding opportunities to support global work.
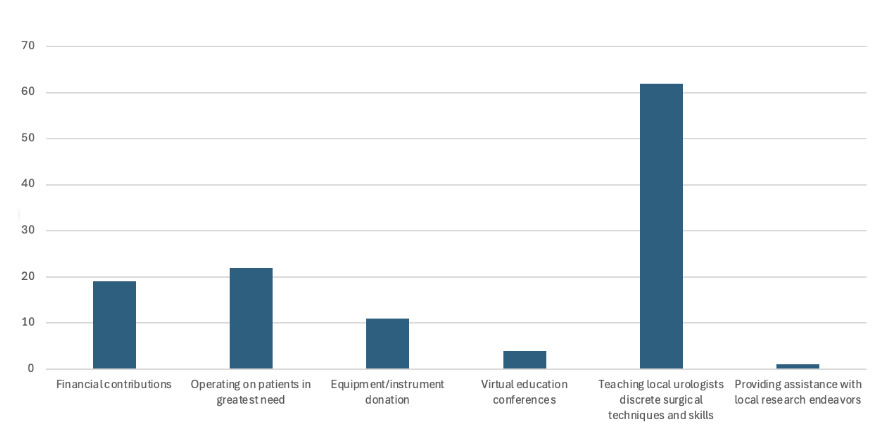
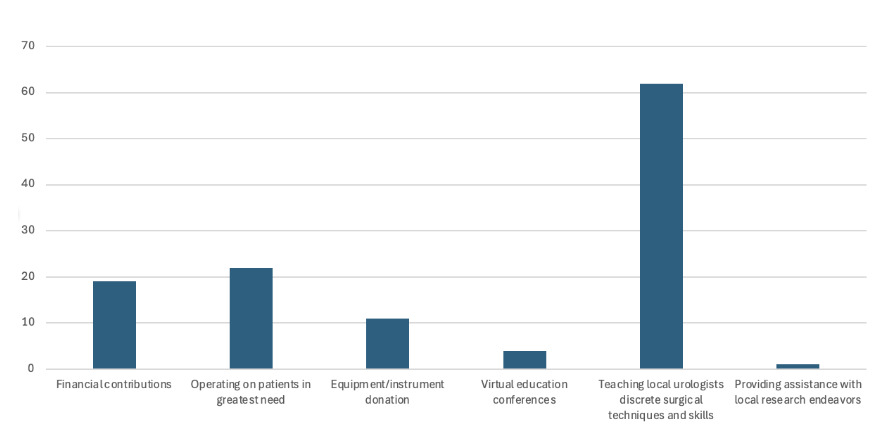
Respondents who had participated in global health activities reported generally positive outcomes, with 80% indicating at least a moderately positive impact on both patient care and training of local providers. Notably, volunteers were significantly more likely to report a “very significant” impact on patient care (27%) than on local training (18%) (p = 0.001). When asked to rank the most impactful modes of contribution to LMICs, “teaching local surgeons” was rated highest, while “aiding in research” was rated lowest (p < 0.001; Figure 3). On average, the importance of educating and building surgical capacity was rated significantly higher than supporting local research (p < 0.001).
Interest in volunteering abroad was high, with 68%, 78%, and 63% of respondents interested in operating, teaching, and participating in regular virtual education conferences, respectively. 77% percent of respondents, including 76% of program leadership, felt global work should count as academic or clinical service; 86% thought it should occur during academic or clinical time, and 66% supported spending two weeks of non-vacation time annually on this work. Prior volunteer experience did not influence these views (all p-values > 0.05). Both respondents with and without prior experience recommended an average of two weeks abroad per academic year (p = 0.6).
U.S. Trainee Involvement
In total, 53% of respondents (n=64) rated US-based trainee involvement in global urology as “important” or “very important.” Among these respondents, the primary reason for inclusion was for trainees “to learn about need and access to surgery across the globe” and the least important reason was “to perform high volume surgery”. Respondents with prior global experience rated the importance of trainee involvement higher than those without (mean 3.0 vs. 2.4, p = 0.005). Those opposed to trainee involvement cited a priority to improve access for domestic under-resourced populations first, as their primary rationale. Table 2 displays the results of regression models evaluating factors associated with promoting U.S. trainee involvement. Support for trainee involvement was higher among those in smaller departments, those with prior global experience, and those supporting capacity and education abroad (all p values < 0.05). Respondents with prior volunteer experience (OR 4.2, p =0.001), those with interest in growing surgical capacity abroad (OR 8, p < 0.001), and those interested in performing surgery abroad (OR 4.2, p = 0.02) were more likely to support trainee involvement, whereas those interested in teaching surgery abroad were significantly less supportive (OR 0.2, p < 0.05).
Discussion
Concerted efforts and collaboration between surgeons in LMICs and those in high-income countries is critical to advancing care for the estimated that 5 billion people worldwide that lack access to affordable surgery.9 While several studies have evaluated the perceptions and relationships of surgeons across countries,10–12 there is a lack of research on this topic among urologists. This study offers one of the first examinations of academic urologists’ experiences with and attitudes toward global urology initiatives, filling a gap in the broader global surgery literature that has historically centered on general surgery. Our findings demonstrate substantial engagement in global health among respondents, particularly in areas of education and surgical capacity-building, a substantial interest in expanding opportunities for involvement, and a strong endorsement of institutional recognition for global work as academic or clinical service.
Importantly, our findings demonstrate that interest in global work is not limited to prior volunteers. Even urologists without global experience called for legitimacy of such work and recommended protected time to pursue it. This suggests a need for institutional support for international surgical endeavors. Responses emphasized the importance of teaching and capacity-building abroad as opposed to episodic surgical care or research, aligning with principles of sustainability and local empowerment.1
Our findings also reveal a key tension in operationalizing global surgery initiatives—particularly regarding trainee involvement. While just over half supported including U.S.-based trainees, this support was not universal. Notably, urologists most interested in teaching abroad were significantly less likely to endorse trainee participation. This paradox suggests that trainees may inadvertently compete with efforts to educate local providers, highlighting the challenge of balancing education for visiting trainees with sustainable local capacity-building. This insight challenges the assumption that trainee involvement is inherently beneficial and underscores the need for programs that are intentional, context-specific, and aligned with local partners’ priorities.
Another notable finding was the consistently low value assigned to supporting research in LMICs. Despite the global health community’s increasing emphasis on the importance of locally driven research for sustainability and health system strengthening,13 many respondents ranked research as the least impactful contribution. This perception likely reflects a disconnect between academic urologists’ traditional scholarly activities and the broader goals of global health equity. Addressing this disconnect will require targeted educational efforts and increased visibility of successful, collaborative research initiatives led by LMIC partners.
These results should be interpreted in the context of ongoing structural barriers to global health participation. More than two-thirds of those who had volunteered abroad had done so using personal funds, and only about half had received any departmental or institutional support. As academic urology seeks to engage more meaningfully in global surgery, it is important for leadership to consider developing formal funding pathways and allocate protected time for these programs. Based on the consensus apparent in our results, we recommend an allotment of 2 weeks per year of non-vacation time for international volunteer work. In addition, recognition of volunteer work abroad as clinical or academic service, to be counted towards academic promotion, was a view shared among the large majority of respondents, including those who hold leadership positions. Such recognition would not only help dismantle structural barriers by legitimizing this work within academic metrics but also encourage greater faculty participation and foster a culture of international service and collaboration.
Other surgical societies in the United States have established global divisions that work to expand surgical access, build international partnerships, and strengthen education in low-resource settings. For example, the American College of Surgeons (ACS) has a Committee on Global Engagement through the ACS Health Outreach Program for Equity in Global Surgery (ACS HOPE). This committee focuses on developing policies that support global surgery, creating educational resources for international learners, and supporting long-term, sustainable international surgical training programs.
However, no comparable division exists within the American Urological Association (AUA). Establishing a dedicated AUA division committed to fundraising and fostering collaborative global efforts would represent a meaningful step forward. As demonstrated in this paper, numerous individuals from a variety of institutions are willing to donate their time, financial resources, and expertise to global urologic work. A centralized, coordinated effort within the AUA to advance global urologic care could amplify these individual contributions and ultimately lead to more sustainable and effective outcomes.
Our study complements prior qualitative work and aligns with calls for academic institutions to treat global engagement as core to academic medicine.14 Additionally, the interest among 68% of respondents in participating in virtual education programming for LMIC surgeons highlights a growing opportunity to support partners longitudinally, even outside of on-site programs.15,16 Unlike short-term surgical trips, virtual education platforms allow for consistent engagement, minimize disruptions to local health systems, and enable bidirectional knowledge exchange. As global urology moves forward, virtual mentorship and digital surgical education may become central pillars of ethical and impactful international collaboration.
This study has several limitations. First, there likely exists a selection bias towards faculty with an interest in global surgery, with more engaged or opinionated individuals potentially overrepresented. Second, the survey did not include perspectives from urology trainees or LMIC collaborators—key voices for designing equitable and effective programs. Future research should incorporate these perspectives and to align program development with volunteers and communities.
Conclusion
This study highlights both the enthusiasm and the challenges surrounding global engagement within academic urology. While respondents demonstrated significant interest in education, capacity-building, and the institutional legitimization of global work, persistent structural barriers—including limited funding, lack of protected time, and inadequate recognition in promotion pathways—continue to impede participation. The ambivalence toward trainee involvement and the undervaluing of research underscore the need for intentional, partner-driven program design that prioritizes sustainability and equity. Expanding virtual education and mentorship offers a promising avenue to strengthen long-term collaborations without disrupting local systems. Ultimately, advancing global urology will require academic institutions to not only acknowledge global engagement as integral to their mission but also to invest in the infrastructure, recognition, and partnerships necessary to make this work impactful and sustainable.
Conflict of Interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.