Introduction
In an era where trauma cases and life-threatening emergencies are becoming increasingly common, the ability to intervene efficiently is essential.1 Radiology plays a vital role in diagnosing and managing patients, particularly in acute care settings where pressing decision-making is required, while also extending to routine inpatient and outpatient practice.
Importance of Radiology in Acute Surgical Patients’ Assessment
In hospital emergency rooms, surgical residents are often the first care providers to come in contact with patients.2 Given this responsibility, it is crucial for all surgical residents to have good radiological education and skills to be able to interpret imaging and handle patients in a timely manner. Radiology also plays a significant role in the clinical assessment of patients in outpatient clinics and inpatient floors.3
Previous studies have demonstrated the importance of radiological skills in surgical residents. In acute settings where radiologists may not be readily available, surgeons must independently interpret imaging, which significantly impacts patient safety and outcomes.4,5 Due to the impracticality of requesting a radiologist to perform a Focused Assessment with Sonography for Trauma (FAST) on multi-trauma patients, it is important for the first responders, whether surgical residents or emergency doctors, to learn this skill.5 Surgeon-performed FAST examination has proven both accurate (99.4%) and specific (99.7%).6
Current Curriculum and Gaps in Training
Despite the clear importance of radiology in surgical practice, there are significant gaps in radiological education within surgical residency programs. The American Board of Surgery (ABS) emphasizes the significance of residents’ competency in utilizing and interpreting diagnostic images in patients’ care.7
However, currently, the ACGME neither mandates a formal radiology rotation for surgical trainees nor provides a standardized program to enhance their imaging interpretation abilities.4,8,9 Consequently, most surgical residency programs lack a formal radiological curriculum to ensure that residents will be able to interpret images efficiently by the end of their training. This lack of structured education leaves most residents to learn imaging interpretation skills informally from senior trainees or attendings, or through elective courses, leading to inconsistencies in training across programs.10 Addressing these gaps requires a complete systematic revision of the radiology curriculum in surgical training, ensuring that residents are equipped with the skills necessary to improve patient care outcomes.
The primary aim of this study is to evaluate the ability of general surgery residents to accurately interpret radiological images and to assess their views on the need for a dedicated radiology curriculum in their residency program.
Methods
This research utilized a cross-sectional survey to assess the radiological interpretation skills and opinions among general surgery residents about the implementation of a formal radiology curriculum into their residency program.
The sample included general surgery residents, ranging from first to fifth year, at three major tertiary hospitals in Amman, Jordan: Jordan University Hospital, King Hussein Medical Center, and Al-Bashir Hospital. Inclusion criteria encompassed residents actively enrolled in their surgical training programs at these institutions.
Data was collected via a questionnaire designed on Google Forms that was validated by a team of expert general surgeons and radiologists.
The survey was divided into four sections.
-
Section 1 collected basic demographic data including gender, year and place of residency, and prior radiological experience in case of previous residency program.
-
Section 2 assessed residents’ comfort levels in interpreting findings among various imaging modalities. After each imaging modality, a question was included to determine whether the residents had been taught about interpreting such findings, and whether it was done through a formal dedication, or an informal session.
-
Section 3 evaluated residents’ ability to interpret various radiological images using twenty-one multiple choice exam style questions. The radiological findings in sections two and three were chosen by general surgery and radiology consultants due to their significance in clinical decision-making. Each question had five answer choices including “normal,” three relevant clinical options and “I don’t know” option. This option was set to encourage honest responses and minimize random guessing. The questions were designed with varying levels of difficulty to reflect the experience differences between residents of different levels.
-
Section 4 gathered residents’ feedback on whether their comfort levels had changed after the exam and their opinion on integrating formal radiological training into their residency curriculum. In addition, it gathered participants’ points of view on receiving a course on e-FAST imaging.
Data collection was conducted over the course of four months, from February-June of 2024. The residents were contacted through phone calls and in person. Those who provided consent received the questionnaire via WhatsApp Messenger. Confidentiality was maintained throughout the study. The Institutional Review Board at Jordan University Hospital, the University of Jordan (IRB-JUH) approved this research (IRB #25113).
Statistical analysis was conducted using IBM SPSS Statistics version 30.0. Descriptive statistics, including means, standard deviations, and percentages, were used to summarize demographic characteristics and participant responses.
To assess the normality of continuous variables, Q-Q plots, histograms, and the Shapiro-Wilk test were examined. The results indicated deviations from normality (p < 0.05 in the Shapiro-Wilk test), justifying the use of non-parametric statistical tests for inferential analysis.
The Mann-Whitney U test was applied to compare confidence levels and test performance with gender and graduation location groups. The Kruskal-Wallis H test was used to compare differences across residency levels, followed by pairwise comparisons using the Mann-Whitney U test for further detailed analysis. The relationship between residency level and both confidence levels and test performance was assessed using Spearman’s rank correlation coefficient (Spearman’s rho).
Additionally, the impact of different teaching methods on exam scores was analyzed using the Kruskal-Wallis H test, with Mann-Whitney U tests for pairwise comparisons when applicable.
A p-value of < 0.05 was considered statistically significant for all analyses. There was no missing data in the dataset, ensuring a complete analysis without the need for imputation or exclusion of cases.
Results
Demographics
Out of a total of 250 general surgery residents across all three major hospitals, 146 (58.4%) residents responded. Of the 250 residents, 49 were female and 201 were male. Table 1 below summarizes the demographic data of the 146 participants.
Of the participants, 105 were male residents (71.9%), and 41 were female residents (28.1%). Postgraduate year (PGY) residents were categorized into junior (PGY1–PGY2), mid-level (PGY3), and senior (PGY4–PGY5) groups. Almost two-thirds earned their medical degrees from universities in Jordan.
Pretest Comfortability Level
In the pretest section of the survey, residents were asked to rate their comfort level in interpreting different imaging modalities using a Likert scale from 1 (Very Uncomfortable) to 5 (Very Comfortable). The calculated mean of these Likert comfortability scores and their standard deviations, for each imaging modality are demonstrated in Table 2.
Participants reported the highest comfortability in interpreting X-ray images (mean = 4.00, SD = 0.61), followed by CT images (mean = 3.67, SD = 0.77), MRCP/MRI images (mean = 3.24, SD = 1.10), and ultrasound images (mean = 2.82, SD = 1.03). The lowest comfortability was observed for intraoperative cholangiogram images (mean = 2.43, SD = 1.25).
Gender Differences
No significant differences were found between male and female residents in terms of subjective comfortability before the exam (pretest) in all imaging modalities combined. The mean comfortability score was 3.50 for males and 3.54 for females, (p = 0.894).
Residency level differences
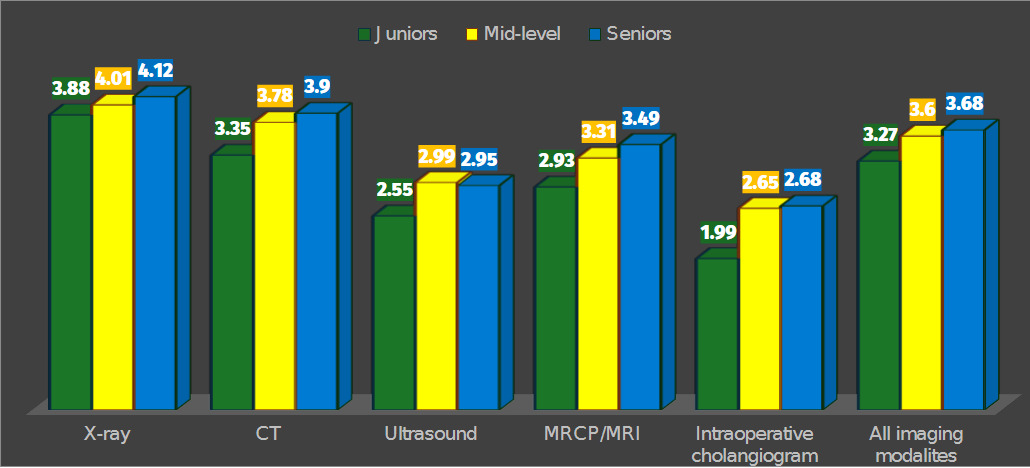
The correlation coefficient was calculated (p < 0.001) for the relationship between residency level and the reported comfortability level.
_in_interpreting_di.png)
CT scans demonstrated the largest variation in comfort levels across residency stages (p < 0.001), with senior residents reporting significantly higher confidence (mean = 3.90) compared to junior residents (mean = 3.35). Similarly, the level of comfort in interpreting intraoperative cholangiograms (p = 0.004) and MRCP/MRI images (p = 0.005) increased significantly with increasing experience. For ultrasound and X-ray interpretations, no statistically significant differences in comfort levels were observed between training levels (p = 0.075 and p = 0.105). However, when analyzing all imaging modalities collectively, a clear upward trend in comfort was noted with increasing experience (p < 0.001), with mean scores rising from 3.27 among junior residents to 3.68 among senior residents.
Results of the Test
Overall Scores and Accuracy Rates
Overall performance across all imaging modalities was 56.98%. When analyzed on a spectrum, X-ray interpretation demonstrated the highest accuracy at 80.53%, followed by CT (54.38%), MRCP (51.37%), and ultrasound (42.33%). The lowest accuracy was observed for intraoperative cholangiograms, with a performance rate of 23.29%.
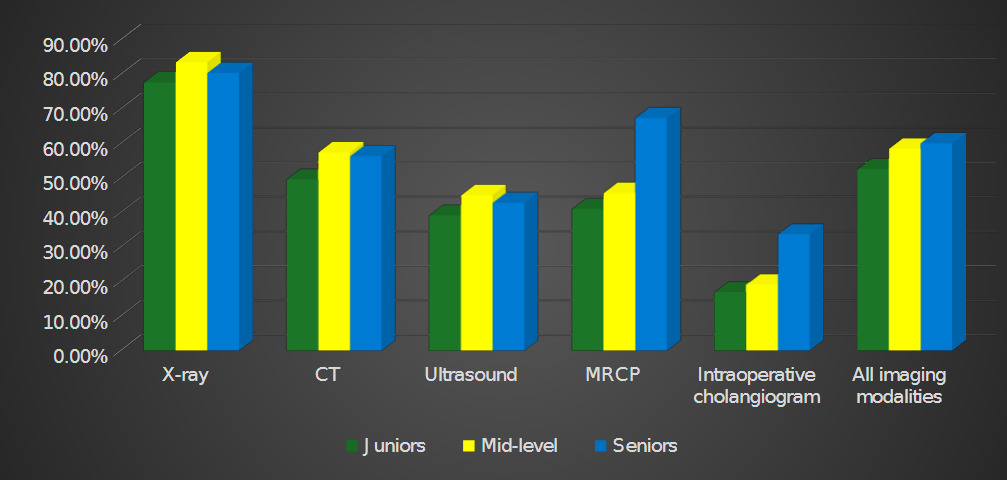
Performance by Residency Level
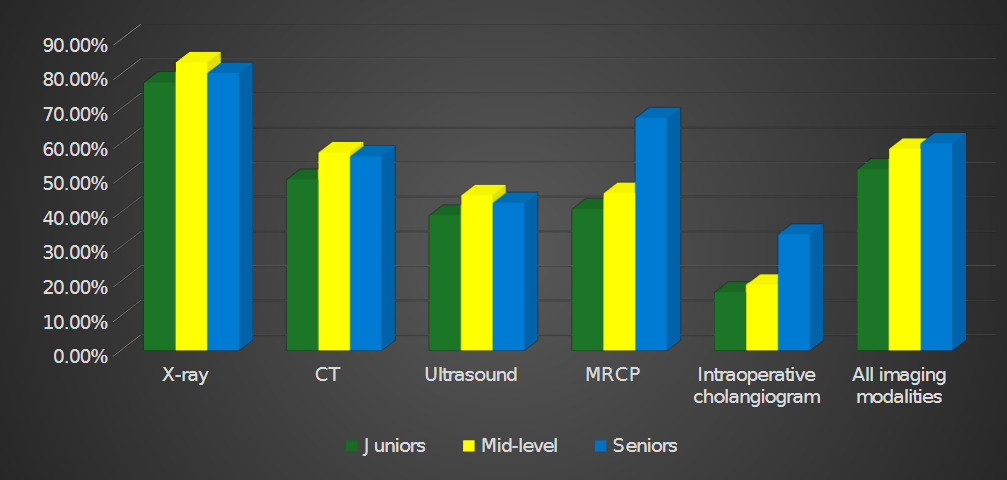
The correlation coefficient was calculated (p = 0.031) for the relationship between residency level and exam performance. Mid-level residents showed higher accuracy rates in X-ray, CT, and ultrasound interpretation compared to other groups (Figure 1). However, the differences across residency levels were not statistically significant (p = 0.239, 0.282, and 0.422, respectively). Senior residents performed significantly better in interpreting MRCP and intraoperative cholangiogram images, with p-values of 0.001 and 0.032, respectively. Senior residents outperformed mid-level residents in both modalities (p = 0.006 and 0.047, respectively).
Gender Differences
Female residents scored slightly higher on average (Mean = 12.76, SD = 3.59) compared to male residents (Mean = 11.66, SD = 3.63), but this difference was not statistically significant (p = 0.083).
Posttest Confidence Level
47.9% of residents reported no change in confidence, 37.7% were uncertain about any changes in their confidence levels, and 14.4% showed a decrease in confidence following the exam.
A significant correlation was found between increasing seniority and confidence level change (p = 0.010).
Teaching Methods Analysis
Teaching Methods Across Imaging Modalities
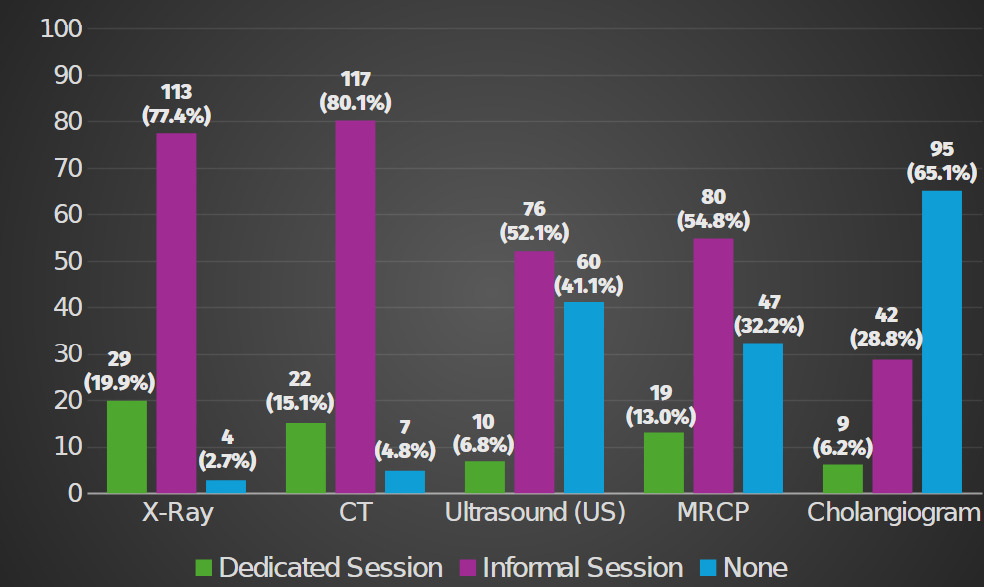
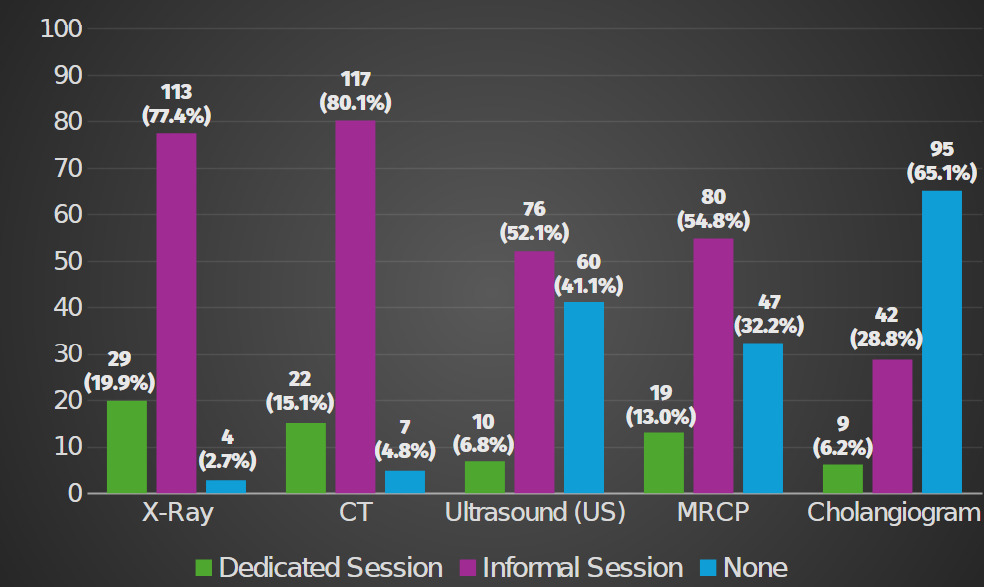
Most participants reported either formal or informal instruction for all modalities except cholangiogram interpretation, in which 65.1% had never received any teaching (Figure 3). Informal teaching was the most common teaching method across the four other imaging modalities (p < 0.001). Ultrasound showed the second highest gap in training, with 41.1% reporting no prior teaching, compared to only 2.7% for X-ray and 4.8% for CT interpretation
Impact of Teaching Methods on Diagnostic Accuracy
Residents who received formal or informal instruction in interpreting X-ray and MRCP images demonstrated significantly higher accuracy than those with no prior teaching (X-ray: p = 0.018 and p = 0.021; MRCP: p = 0.004 and p < 0.001). However, there was no significant difference between formal and informal teaching for either modality (X-ray: p = 0.346; MRCP: p = 0.938). For CT, ultrasound, and cholangiogram images, performance did not differ significantly across teaching methods (p = 0.596, p = 0.447, and p = 0.465, respectively).
Perception Towards Enhancing Radiological Training
Enhancing the Radiological Program
93.9% of the residents agreed on adding a radiology assessment tool to evaluate their competency. 93.1% supported integrating radiology sessions into the curriculum. When asked about the session frequency preference, 67.8% preferred monthly sessions, while 15.8% favored every three months, 4.2% twice a year, and 8.2 once a year.
Residents ranked imaging modalities based on their perceived importance in training, with the X-ray being the most imaging modality checked as the first choice (57.53%), followed by CT scans (25.34%), FAST (14.38%), and ultrasound (2.06%). The least selected modalities were MRCP and MRI at 0.69%, and none selected intraoperative cholangiogram as their first choice.
Respondents were asked to indicate their preferences for who should conduct learning sessions, with the option to select more than one answer from the following groups: radiology consultants, surgery consultants, radiology residents, and surgery residents. 137 out of 146 (93.8%) chose radiology consultants as their preferred instructor, and 111 out of 146 (76%) chose surgery consultants.
eFAST course
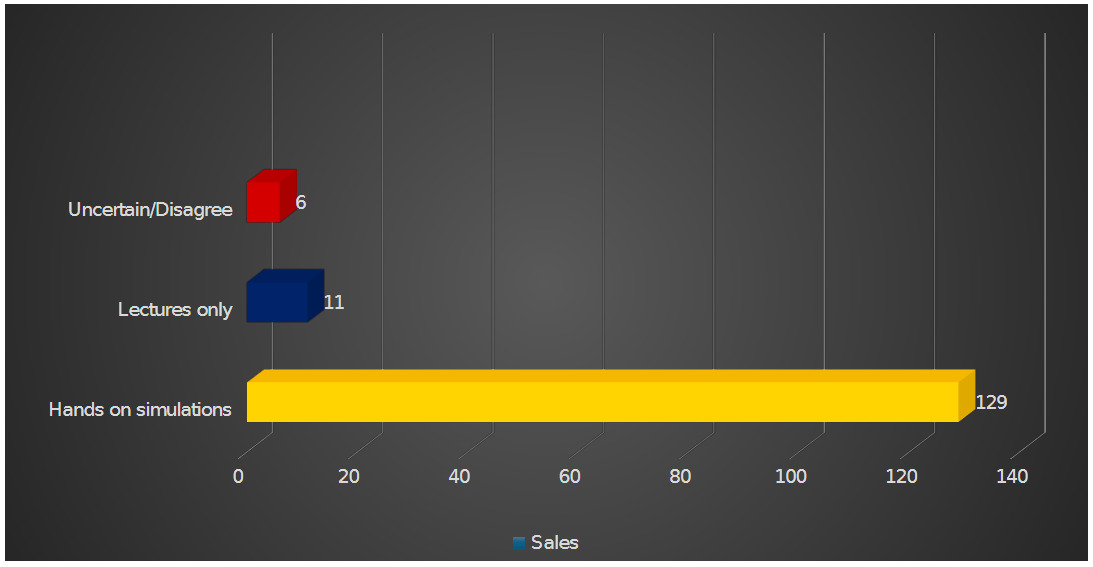
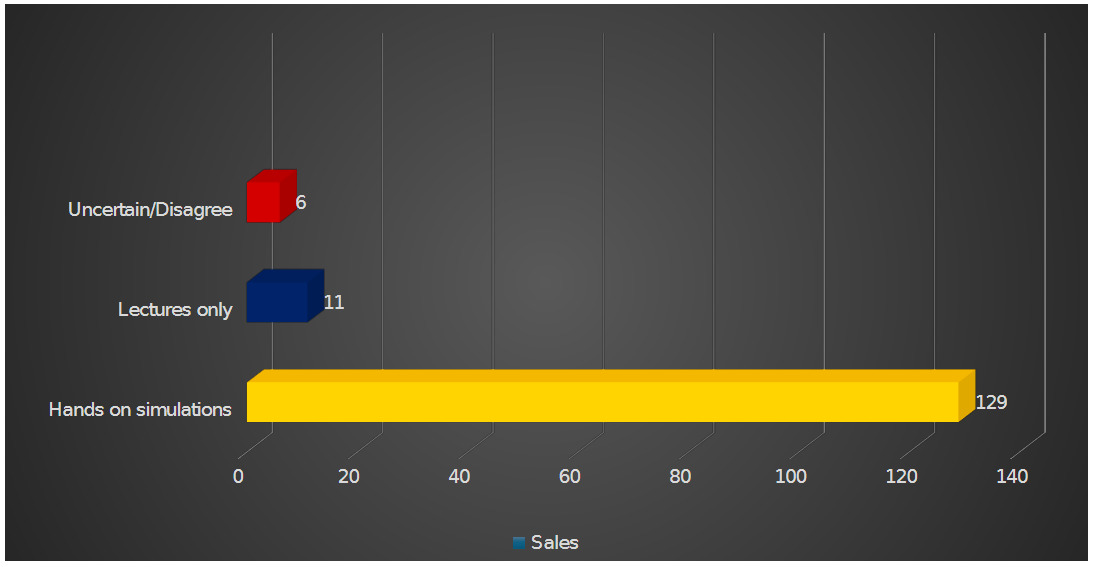
The residents were also surveyed regarding their support for receiving eFAST course. The majority, 88.4% (n = 129), endorsed a combination of lectures and simulations (Hands on). 7.5% (n = 11) favored lectures only, 1.4% (n = 2) remained uncertain or neutral, and 2.7% (n = 4) expressed opposition to the course.
Discussion
Surgical residents play a crucial role in interpreting diagnostic imaging to guide patient care, especially in acute settings. This study aimed to analyze their interpretive abilities, considering different imaging modalities as well as residency level. The even distribution across junior, mid-level, and senior residents allowed for a balanced comparison of interpretive skill progression.
Our study confirmed a significant gap in radiological assessment among the general surgery residents across three main residency programs in Jordan. The results revealed notable variations in accuracy between imaging modalities. While most participants correctly identified multiple findings on X-rays, their performance declined with ultrasound and intraoperative cholangiogram images. X-rays and CT scans had the highest accuracy rates at 80.53% and 54.38%, respectively. Their widespread use in both routine clinical practice and emergency settings contributed to the residents’ familiarity with these modalities. Likewise, studies on surgical residency programs in the United States have highlighted deficiencies in radiology training. Aziz et al.4 reported challenges for residents in interpreting certain imaging studies, while Eid et al.11 noted a significant misdiagnosis rate when comparing general surgery residents to radiologists.
Ultrasound remains a critical tool in surgical decision-making, predominantly in trauma or abdominal cases.12 Yet, 41% of our participants reported having never received training in ultrasound or FAST scans. Studies in other regions, including Canada, have highlighted a similar trend, where a large proportion of general surgery residents lacked formal training in interpreting FAST scans, despite their significant role in trauma management.13,14 These findings emphasize the need for targeted training in less commonly used imaging modalities that require more specialized interpretation.
Our data showed a clear correlation between residency level and improved interpretive accuracy (p=0.031). Senior residents exhibited higher skills specifically in interpreting cholangiogram and MRCP images (p=0.001, p=0.032 respectively), reinforcing the role of training exposure in developing these skills. This aligns with previous studies, such as Aziz et al.'s4 which found that radiological interpretation improves with training and experience, with 89% of PGY-5 residents achieving accurate interpretations compared to 61% of PGY-1 residents. Furthermore, Eid et al.15 reported that medical students performed comparably to junior general surgery residents in X-ray interpretation, suggesting minimal improvement in radiological knowledge during the early years of training. These studies further stress the importance of addressing the deficit early on and implementing structured radiological education for residents as soon as they start residency.
It is also important to consider how these results line up with their pretest self-perception. The highest confidence was in identifying findings on X-ray images, while the lowest was in interpreting intraoperative cholangiograms, a pattern that mirrored their diagnostic accuracy. Interestingly, although the residents reported high confidence in their ability to interpret images, with an average self-assessment of 79.5%, more than half of them experienced a shift in confidence after the exam. This discrepancy suggests that surgical residents may overestimate their interpretive abilities, which should be mitigated to avoid impacting their diagnostic decision-making and skill development.
A key finding of our study is the lack of a formal diagnostic radiology curriculum across general surgery residency programs in Jordan. The majority of surgical residents’ radiological knowledge gained during residency is through discussing cases and images of patients with colleagues and superiors informally. This was consistent with a multicenter study done by Butler et al.16 where 82% of residents shared that teaching from their senior colleagues was the most important contributor to their knowledge in radiology.
To address this gap in the surgical residency program, incorporating a dedicated radiology curriculum is critical. Suggested enhancements include simulation systems and workshops led by radiologists, which have been shown to improve diagnostic accuracy and procedural skills.13
Our study revealed that most residents (93.9%) agreed on the significance of integrating radiology into their curriculum and its importance in their daily clinical practice. Likewise, Aziz et al.4 found that a significant number of residents (63.7%) supported the introduction of inbuilt radiology rotations, with 66.3% believing that imaging interpretation should be a core surgical competency. Residents identified X-rays, CT scans, FAST and ultrasound as the most critical modalities for inclusion in their training. Implementing these measures will not only improve their radiological skills but also boost their confidence in making independent decisions under any circumstance, especially in emergencies and when radiologists are unavailable.16
Strengths and Limitations
A key strength of our study is its multicenter approach. By including residents from three major hospitals in Amman across all residency levels, we were able to capture a diverse range of experiences and perspectives from each of their residency programs. To the best of our knowledge, this is the first assessment of general surgery residents’ comfort and interpretation skills across multiple imaging modalities, including images from both trauma and non-trauma settings, in Jordan and the broader MENA region.
However, it is important to acknowledge potential limitations, including the sample size and response rate. These factors may affect the representativeness of our findings in relation to the broader population of general surgery residents and influence the generalizability of the results across Jordan and other countries.
It is also worth noting that although female residents involved in this study were less than half the number of their male colleagues, their participation rate was markedly higher: 83.7% of all female residents contacted participated, compared to only 52.2% of the male residents. This may reflect greater engagement of female residents in research activities, a trend that prompts further investigation.
Conclusion
This study emphasizes the need for formal radiology education in general surgery residency programs to enhance interpretive skills and patient care, and the residents themselves strongly supported this idea. Implementing tailored sessions by experts in X-ray, CT, and ultrasonography (especially FAST) can address existing training gaps and improve patient care outcomes.
Further research with larger and more diverse samples is needed to enhance the generalizability of our findings and evaluate the long-term impact of structured radiology training on resident competence and patient outcomes. Nonetheless, this study lays a solid foundation for future efforts aimed at optimizing radiology education within surgical residency programs.