INTRODUCTION
Research activity is a critical part of the field of orthopaedics, contributing to the advancement of physicians’ medical knowledge and novel ways to improve patient care. During residency training specifically, the Accreditation Council for Graduate Medical Education (ACGME) requires all programs to have a scholarly component.1 In addition, the American Board of Orthopaedic Surgery (ABOS) specifies in their rules and procedures for residency education that programs must provide exposure to research.2 Neither of these bodies further specifies the research requirement much further than this description. As a result, individual programs can interpret these requirements regarding exposure, productivity, and support for resident led research.
Academic productivity has been heavily prioritized by prospective orthopaedic surgery residency applicants. From 2022 to 2024, NRMP data demonstrates the average number of abstracts, publications, and presentations for matched orthopaedic surgery applicants increasing from 16.5 to 23.8.3 A gap in training in the form of a ‘research year’ has grown in popularity among medical students to keep up with this research demand.4 As medical students enter residency with more research experience, this increased productivity has yet to be described with regards to its effect on productivity during residency. Regardless, research productivity remains important for residents applying into fellowships. With this stark upwards trend in academic productivity prior to matriculation into training, the support available to residents during training may influence their ability to maintain productivity.
Barriers to research participation have been cited related to lack of dedicated time, lack of financial support, inadequate mentorship, and unfamiliarity with the research administrative process, including Institutional Review Board (IRB) approval process. One prior survey comparing research funding between residencies demonstrated programs with more funding and staff support had the greatest research productivity.5 Implementation of a resident research curriculum, including focus on yearly milestones, support staff, mentoring, lab usage, and dedicated time for research has been demonstrated to significantly increase the number of research grants attained and peer reviewed publications.6 While some of the current challenges to attaining greater research productivity during residency may be modifiable with an increase in available resources, the level of support for resident led research is not uniform across United States (US) based programs. Therefore, this study aims to explore the level of support provided by US orthopaedic departments in terms of human resource, trainings, time allotment and funding for their residents to perform, present, and publish research.
METHODS
This study was a prospective survey disseminated to all US based orthopaedic surgery residency program coordinators, both directly via email, and indirectly via the Association for Residency Coordinators in Orthopaedic Surgery. The survey was secondarily disseminated to all US based orthopaedic residency program directors directly via email. Emails were obtained from publicly available websites for each program.
Our study did receive Institutional Review Board approval through the University at Buffalo. The anonymous survey was built, data collected and managed using REDCap electronic data capture tools hosted at the University at Buffalo. REDCap (Research Electronic Data Capture) is a secure, web-based software platform designed to support data capture for research studies, providing 1) an intuitive interface for validated data capture; 2) audit trails for tracking data manipulation and export procedures; 3) automated export procedures for seamless data downloads to common statistical packages; and 4) procedures for data integration and interoperability with external sources.7 Written informed consent was obtained prior to accessing the online survey from all participants. Participants were given one month to complete the survey, with one reminder sent out at 2 weeks after the initial invitation to maximize response rates.
Our survey queried key areas of departmental support for resident led research at each individual program, including presence of research staff, resources for attending conferences, and funding for research publications (Supplement 1). Open answer responses were accepted to qualify answers and to additionally inquire about specific barriers to resident led research, identifying both barriers within and external to each surveyed orthopaedic department.
Statistical analysis was conducted using R studio version 4.2.3 (Boston, MA, USA). P value < 0.05 was considered statistically significant.
RESULTS
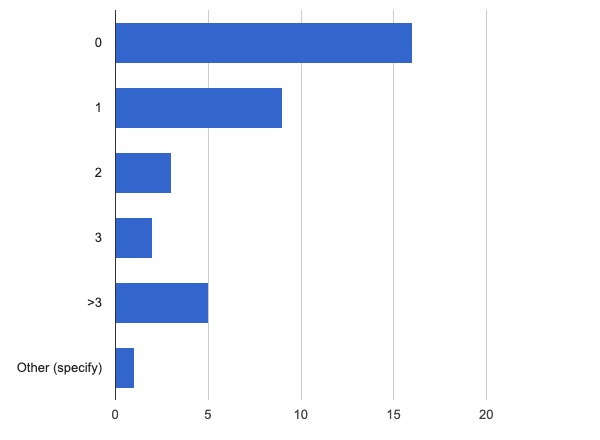
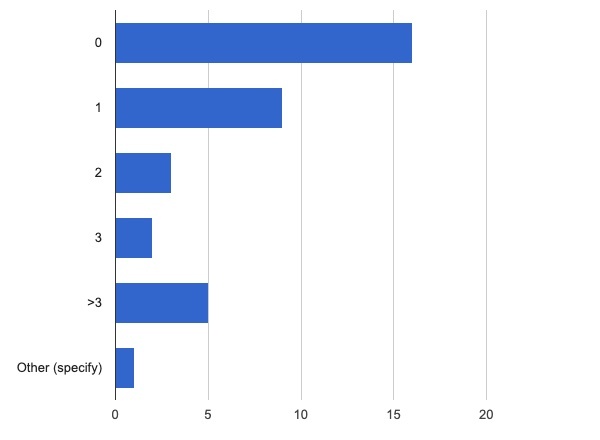
36 of 207 programs responded, with a response rate of 17.4%. Of these, 38.9% (14/36) reported access to dedicated personnel specific for resident led research through their department; 25% (9/36) reported only 1 staff member dedicated to resident led research (Figure 1).
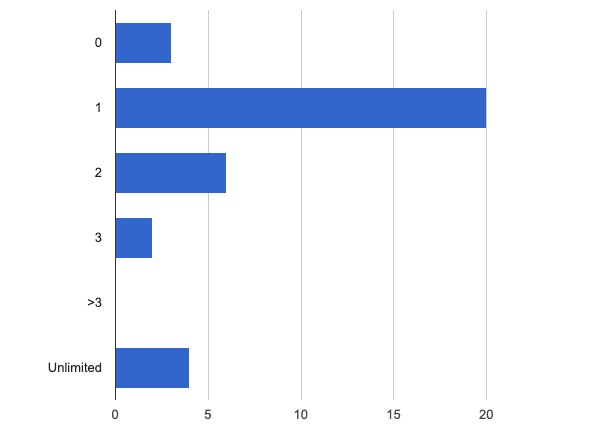
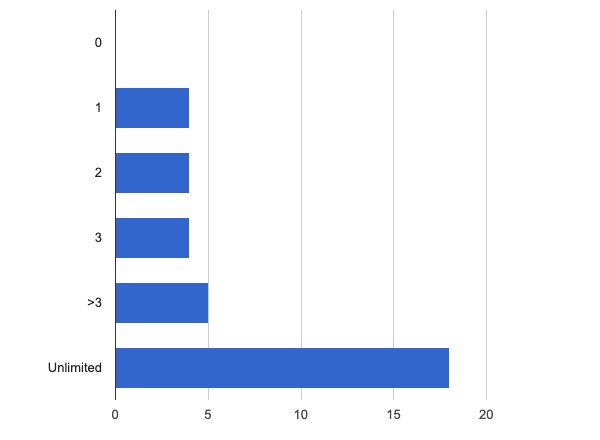
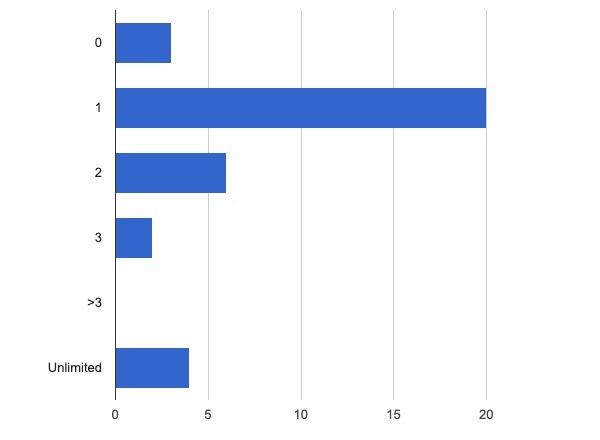
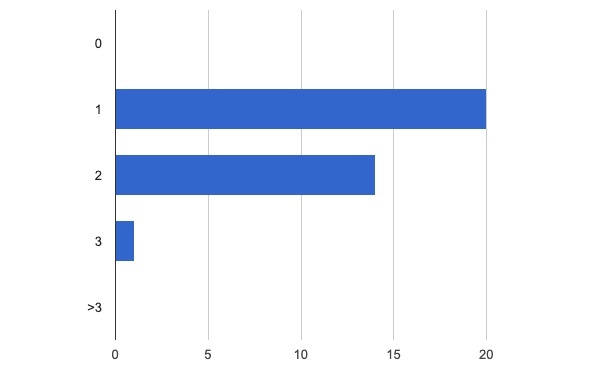
57.1% (20/36) reported that residents were allowed time excused from clinical duties to attend one conference annually without presenting research. 11.4% (4/36) reported unlimited time excused for attending conferences without presentation annually (Figure 2). Conversely, 51.4% (18/36) reported unlimited time excused for residents presenting research at conferences annually (Figure 3).

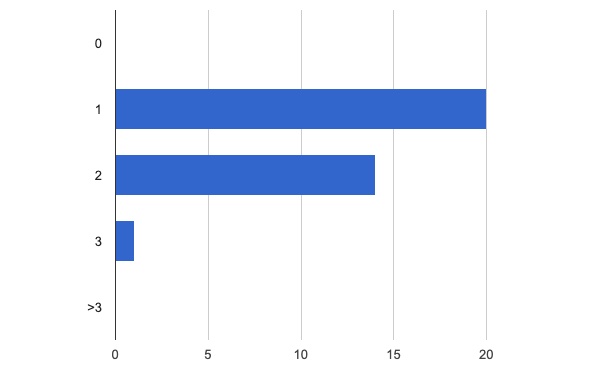
Most programs (94.4%, 34/36) reported funding available for residents to attend conferences, including reimbursement for the cost of conference registration, travel, lodging, and a food stipend in most cases (69.4%, 25/36). 6 programs reported specific other stipends, ranging from $1000-2500 per conference. Residents were reported to attend on average one (57.1%, 20/36), two (40.4%, 14/36) or three (2.9%, 1/36) conferences annually (Figure 4).
Most programs (72.2%, 26/36) reported funding available for resident publication through their department, with the majority (54.5%, 18/36) reporting unlimited funding available for publication of resident led research.
Intradepartmental barriers to research were identified as related to lack of administrative support from dedicated research staff by 15 programs and related to lack of funding by 6 programs. With regards to identified barriers outside of their own department, 8 programs cited difficulty obtaining funding for resident led projects, 4 programs cited frustrations with cumbersome IRB approval processes, and an additional 4 programs cited limitations due to lack of centralized administrative leadership and access to statistical analysis.
DISCUSSION
The increase in research productivity in successful orthopaedic applicants in recent years is well documented.8 These trends may be partially explained by an increase in popularity of dedicated research time prior to matriculation into residency training,9 which has been demonstrated to positively influence successful matriculation into residency training through the match.10 Dedicated research fellowship programs targeted towards medical students have also increased in number,4 and research productivity after participation in formal research fellowship programs has demonstrated increased odds of matching into orthopaedic residency.11 As research productivity continues to be prioritized amongst orthopaedic surgery applicants, similar trends may be seen amongst residents; in fact, 2 or more publications prior to residency is associated with more publications during residency training.12 Academically productive medical students are additionally more likely to apply to fellowship after residency,13 and residents applying to fellowships and pursuing practice in academic settings have been noted to have a significantly higher academic metrics.13 Scholarly productivity remains important in successful fellowship match; one analysis demonstrated increases in publications among sports medicine fellowship applicants in the Northeast from 2010-2017, among whom applicants with more publications were more likely to match.14
With regards to research requirements during training, the ACGME requires all residency programs to have a scholarly component, including resident participation in sponsored research, publication of an article through peer reviewed publication, presentation at a regional or national meeting, or participation in a structured literature review.1 The ACGME additionally stipulates that “the sponsoring institution and program should allocate adequate educational resources to facilitate resident involvement in research.”15,16 However, without more specific definition of “adequate educational resources,” interpretation of both the scholarly requirement and subsequent support is not uniform between training programs, and varies greatly with regards to available resources, dedicated time, structure, and expectation of residents required scholarly activity.17 However, institutional initiatives have been described that may positively influence orthopaedic clinician-scientist career development, including facilitation of research teams to allow for successful collaboration, protection of time devoted to research, and provision of research infrastructure at the department level.18
Previous studies have demonstrated the importance of dedicated research time during residency training.19 Implementation of a dedicated research rotation during residency has been shown to substantially increase resident and faculty publication rate, with one program citing an increase in resident publications from 2 to 26, and faculty publications from 22 to 25 after implementation of the rotation.20 Restructuring of an established resident research rotation including appointment of 2 clinical orthopaedic faculty codirectors, development of a revised curriculum, use of research teams, and a centralized research database at another program was found to significantly increase the research productivity of graduating orthopaedic surgery residents and associated clinical faculty.21 The establishment of structured research teams as described by Konstantakos et al.22 additionally demonstrated increases in academic productivity by orthopaedic residents, although their impact on faculty productivity was not mentioned.
Most programs included in our analysis cited funding and a lack of a dedicated research staff as the main barriers to resident led research within their own departments. These findings corroborate with previously published literature; in one survey of 69 residency programs, research productivity was associated with a higher research budget and presence of dedicated research assistants.5 Indeed, the top five most productive programs cited their own dedicated research assistant, despite two of these programs not allowing for dedicated research time during training,5 suggesting that an adequate level of administrative support may supersede the importance of dedicated research time. Access to grant funding has been demonstrated to increase resident scholarly output,23 a trend which continues amongst orthopaedic surgical faculty, as increasing scholarly impact correlates with higher levels of funding.24
Concerning trends of declining clinician-scientists, even in the field of orthopaedic surgery, have been described.25,26 The effect of adequate exposure to research training and dedicated resources towards resident led research during training cannot be overstated in its importance towards cultivating these future clinician-scientists. One survey indicated that 65% of orthopaedic clinician-scientists began their research careers before residency, with nearly half undergoing additional specialized training in research.27 Adequate support for resident led research has been demonstrated not only to significantly increase the academic productivity of current clinical teaching faculty of the established programs,20,21 but also may predict future academic success of involved trainees, as scholarly metrics correlate to higher academic orthopaedic faculty rank.28 Indeed, in one survey 42% of orthopaedic residents reported they were certain or likely to perform research during their careers, with primary authorship on a prior manuscript and past research experience associated with greater future research interest; however, residents and program chairs alike indicated that increased funding and protected time were the greatest incentives for participation in research during training.29 Calls for support of orthopaedic clinician-scientists highlight the necessity of strategic funding programs, provisions for research education during medical school and residency training, and financial support including establishment of grants to support pilot experiments, institution of loan repayment programs, and research support for every career level of clinician-scientists.30
Our study data is limited in the power of our survey results based on our response rate. As this was a largely descriptive analysis, and given response rate limitations, power analysis was not included as part of this study. Our nonrespondent rate was also high, with 55 respondents initially accessing our electronic survey, but only 36 consenting to and participating in the survey questionnaire. Of those who chose not to respond to our survey, we did not collect data as to the rationale for nonresponse. As a result, there is a risk of sampling and attrition bias. In addition, there is a possibility of selection bias as programs offering more research support may have been more inclined to participate in our survey. Our study is also limited in that program reputation, funding sources, and location were not queried, limiting our ability to comment on these factors. Finally, as this study represents a pilot survey, no external validation of our questionnaire was performed beyond initial study team member study design meetings. However, our analysis does demonstrate a diverse range of resources available for resident led research, as well as multiple clearly defined barriers to be the focus of future study and intervention.
CONCLUSIONS
There exists no standard between US based orthopaedic residency programs regarding support made available for residents to complete research during training, despite standardized academic requirements from the ACGME. Most programs offer protected time to present research at one conference annually and offer some level of funding support for conference attendance and publication costs. However, lack of research personnel dedicated to support of resident led research was uniformly identified as a barrier to resident led research, both within and external to the programs who responded to our survey, including explicit report of lack of dedicated staff, and associated administrative barriers that could be partially alleviated by dedicated staff.