Introduction
Research is a vital precursor to evidence-based medical practice, specifically in areas of innovation, advancement, and clinical practice guidelines.1 Academic medicine plays a pivotal role in contributing to the body of research literature while training practitioners with the ability to critically examine and perform research throughout their careers. Moreover, resident-driven research has been reported to show improved clinical care and patient outcomes.2,3 Additionally, the orthopedic job market has trended toward seeking more fellowship-trained surgeons,4 such that orthopedic surgery residency graduates are becoming increasingly subspecialized.5 As the competitiveness of orthopedic surgery fellowships continues to rise, there has been an overall increase in the number of publications expected from fellowship applicants.6,7 The impact of scholarly activity in orthopedic residency extends beyond fellowship, as residents who publish peer-reviewed research while completing their training are more likely to continue publishing research throughout their careers as attending surgeons, thus contributing to the ongoing evolution of evidence-based practice.8
Thus, in addition to teaching clinical and surgical practices, it is imperative that an orthopedic surgery residency program supports and teaches trainees about clinical research. Unfortunately, the research curriculum at many orthopedic training programs is severely underdeveloped.9 The Accreditation Council for Medical Education (ACGME) has attempted to emphasize such development by requiring orthopedic trainees to participate in scholarly activity, with the goal of publishing or presenting clinical research during their time as a resident.10 Dedicated research time in orthopedic residency has been shown to be associated with an increase in scholarly productivity.11 Training programs have attempted to improve research productivity by increasing faculty support and expertise, adding research support services, and creating infrastructure for clinical research.12 However, building research capacity can be a difficult feat for residency programs with limited budgets for research, lack of dedicated research staff, and limited time committed solely to research, and programs can be put on probation or ultimately terminated if they do not meet ACGME research requirements.13 Therefore, smaller institutions with limited resources are often investigating ways to find and produce clinical research effectively and efficiently to improve resident training and comply with ACGME requirements.
In 2008, Wright State’s Orthopedic Surgery program developed a dual-track residency program, adding a research-specific track to improve scholarly output at our institution. In addition to the program’s existing track of two categorical residents per year, two additional residents were added to the program each year to participate specifically in a yearlong rotation dedicated primarily to research. The categorical and research tracks have separate National Resident Match Program (NRMP) numbers and are ranked separately by applicants.
The research track is thus a 6-year orthopedic residency including the dedicated research year between postgraduate years 1 and 2. During this year, residents have limited clinical duties to ensure that the majority of their time can be dedicated to research. Research residents are given office space; participate in weekly research meetings with the program director, research director, and available attendings; and travel to present at regional and national professional meetings. The weekly research meetings create an environment where the residents provide updates on projects and receive meaningful feedback and guidance, statistical and data management support, and assistance with generating abstracts and manuscripts for publication. Research residents also maintain clinical skills by participating in two days of clinic each week, spending a day in the operating room, and taking in-house call once every other week. After completion of their research year, residents then continue their training in the traditional fashion.
The research track was implemented to increase the overall time residents had dedicated to performing research, to increase the program’s scholarly productivity, and to ensure ongoing fulfillment of ACGME guidelines for resident participation in research. The dual track has remained in place since its inception in 2008, and we have observed, anecdotally, an increase in program research productivity over the intervening period. The purpose of this study is to formally evaluate the impact of research track implementation on program research productivity, operationally defined here as the publication rate per resident. We compared PubMed-indexed publications of all residents before and after research track implementation to test the hypothesis that the research residency has increased overall program research productivity. A secondary aim was to test whether any effect on productivity was observed not just in research resident publications, but also in the productivity of post-implementation categorical residents as a result of increased research support and infrastructure.
Methods
Ethical approval was not required for this study, since all information on past program resident publications is publicly available and required no interaction with the individuals in question. We collected bibliographic information for all PubMed-indexed, peer-reviewed scholarly articles authored (in any authorship position) by Wright State’s orthopedic surgery residents published between January 1, 1997, and December 31, 2023. Search terms included each resident’s last name along with the residency’s affiliated institutions “Wright State University,” “Premier Health Partners,” “Dayton Veterans Affairs Hospital,” or “Dayton Children’s Hospital,” and variants thereof (e.g., “Dayton VA”). We included all publications that were either published during residency, or where data collection for the publication was completed during residency (identified as having occurred at our institution and/or one of our partner institutions in the affiliations and/or article text). All published articles by each author were examined to ensure they met these criteria. Additionally, we excluded any articles published prior to residency or that were not directly affiliated with one of our training institutions.
Residents and their publications were assigned to one of two groups, either the pre-dual track cohort (pre-DT), from 1994-2007, or the dual-track cohort (DT), consisting of all residents who began their residencies after implementation of the research track (2008-2023). Within the DT cohort, we also coded each resident according to whether they were in the 6-year research track (DT-R) or the 5-year categorical track (DT-C). Because research residents have an extra year to conduct research and publish, we corrected for variation in residency length by adjusting each resident’s number of publications by years in residency, which we called, “publications per residency year” (PPRY).
In addition to variation in residency length, another issue that had the potential to introduce bias to our analyses was the fact that many articles included multiple residents as co-authors. If we counted a multi-authored paper toward each resident co-author’s total and co-authored papers were more common in the DT cohort compared to the pre-DT cohort, then the number of papers counted, PPRY, and thus productivity, could be overestimated in the DT cohort, biasing our results. On the other hand, there are reasons to count a multi-authored paper towards the total of each resident co-author, related to how productivity is quantified, as well as the value of productivity to residents. First, implicit in a multi-authored paper is the concept that each author made significant contributions to the work, and thus added to the productivity the article represents. To only consider an article toward the total of the highest-ordered resident author, for example, would suggest that any remaining residents did not contribute meaningfully to the project and were thus not productive. Second, if one of the goals of boosting resident research productivity is to boost their competitiveness when applying for fellowships, then the total papers they have contributed to, regardless of author order, is likely the most salient variable. This argues for counting each resident’s total number of publications, even if that means co-authored papers are counted on multiple residents’ totals.
To determine whether this approach would bias results, we ran a sensitivity analysis using the same statistical tests described below, but limiting the data so that each co-authored publication was counted toward only one resident’s total, in this case, the resident highest in the author order. Although the overall PPRY totals were lower, the results of this sensitivity analysis were not qualitatively different, in terms of the statistical significance and directionality of comparisons between pre-DT, DT-C, and DT-R resident research productivity, from the results when co-authored publications were counted toward each co-author’s total. Thus, the results presented below reflect the approach where a co-authored paper was counted toward the total for each resident co-author. We assessed productivity in terms of having any publications (yes/no), the average total number of publications per resident, and PPRY.
Statistical Analysis
Statistical analysis was performed in SAS 9.4 (SAS Institute, Cary, NC) with statistical significance set to α=0.05. Descriptive statistics were derived for each variable. Because we specifically hypothesized that the DT cohort would have higher productivity than the pre-DT cohort, where applicable all statistical tests were one-tailed. For the primary hypotheses comparing the pre-DT and DT cohorts, we used Fisher’s exact test to compare frequencies of any vs. no publications, and used independent samples t-tests to compare mean number of publications and mean PPRY. We conducted a secondary analysis breaking the DT cohort into its two constituent groups, DT-R and DT-C, and compared them to each other as well as to the pre-DT cohort. Here, we used nested chi-square tests to compare frequencies of any/no publications, and one-way ANOVA to compare mean number of publication and mean PPRY, with post hoc pairwise tests adjusted for multiple comparisons (Tukey HSD).
Results
The sample included 30 annual cohorts consisting of 96 total residents. We recorded a total of n=134 unique publications over the course of 472 cumulative resident years, resulting in an overall PPRY of 0.28. This figure represents a rate of roughly 1 publication per every 3 resident years. Broken down relative to research track implementation, there were 16 pre-DT cohorts with a total of 37 residents and 186 resident years, and 14 DT cohorts with a total of 59 residents and 286 resident years. Within the DT cohort, there were 27 DT-R residents accounting for 142 resident years, and 32 DT-C residents accounting for 144 resident years. See Table 1 for publication data by cohort.
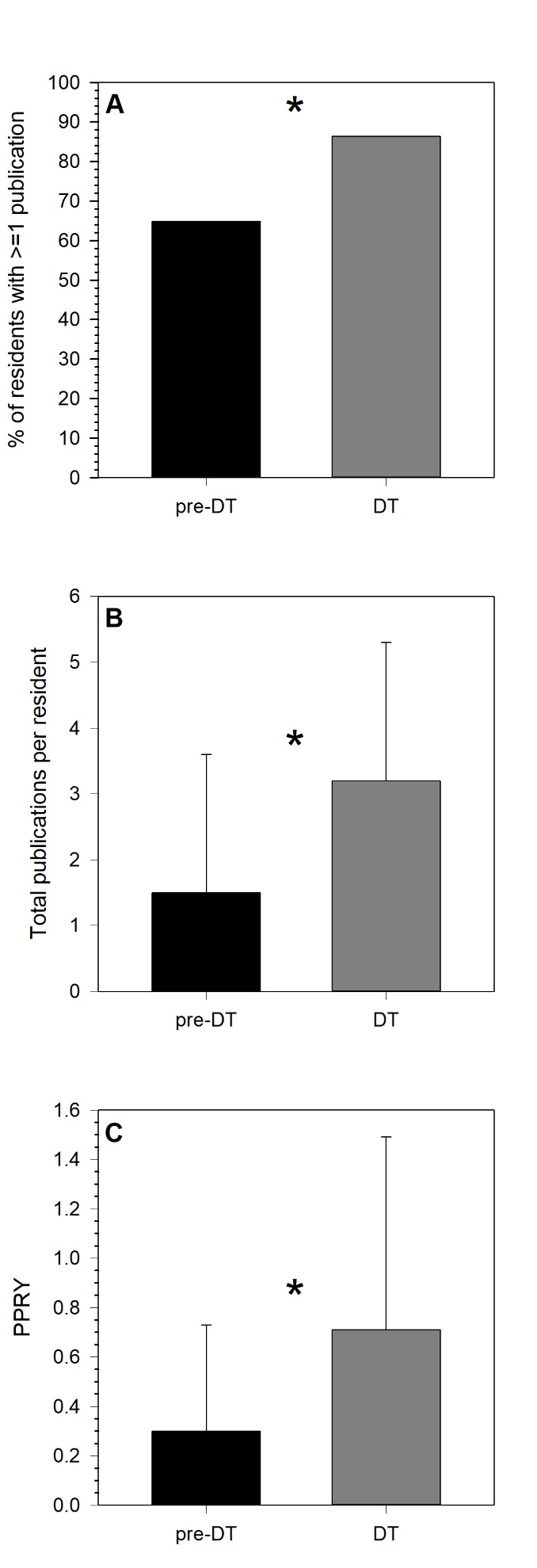
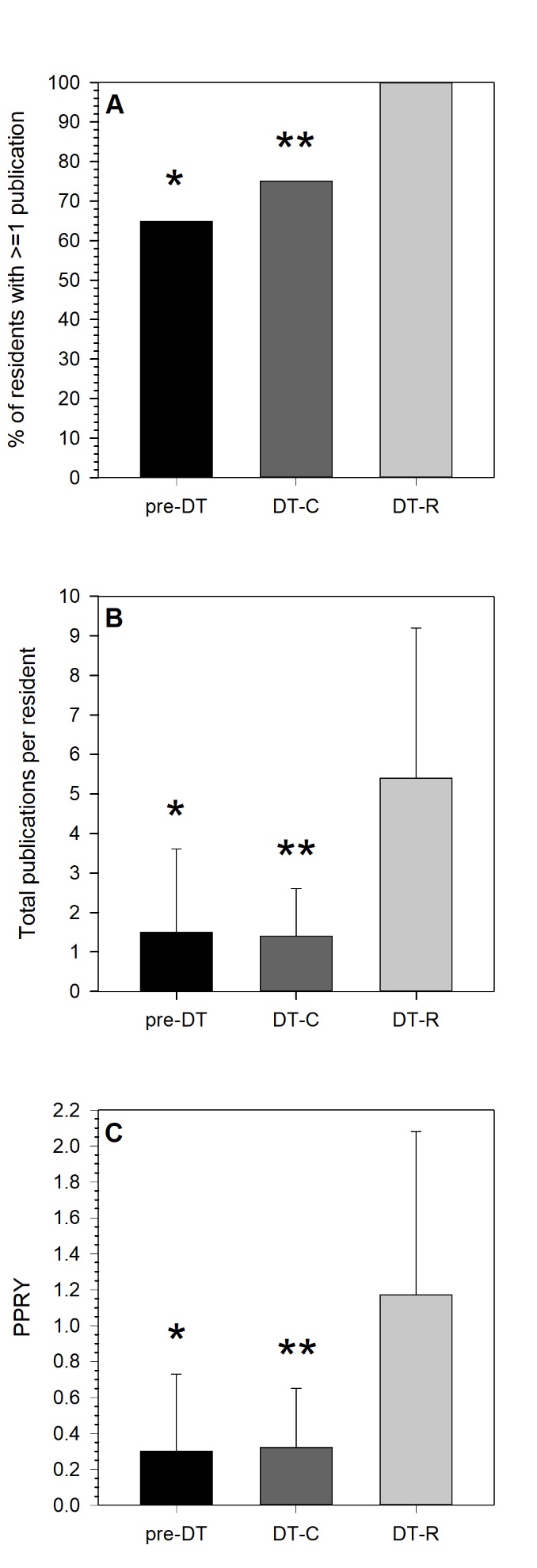
Overall, DT residents were significantly more likely than pre-DT residents to have at least one publication (86.4% vs. 64.9%, respectively; P=0.021), had significantly higher mean publications per resident (3.2±2.1 vs. 1.5±2.1, respectively; P=0.001), and had significantly higher mean PPRY (0.71±0.78 vs. 0.30±0.43, respectively; P<0.001). See Figure 1. Breaking down the DT cohort into its DT-R and DT-C subgroups, there were significant between-groups differences for the frequency of residents with at least one publication (χ2=11.6, P=0.003), mean publications per resident (F=25.1, P=0.001), and mean PPRY (F=21.6, P=0.001). Post hoc pairwise comparisons showed that the DT-R residents were significantly more likely to have at least one publication, had higher mean publications per resident, and exhibited a higher PPRY, compared to each of the other groups (for each, P≤0.005), but the DT-C and pre-DT groups did not differ significantly from each other (for each, P≥0.362). See Figure 2.


Discussion
Our institution’s orthopedic surgery residency program implemented a research track in 2008 that significantly increased the volume of peer-reviewed publications produced by residents. The track included two additional residents per class who participate in a year dedicated to research after their first postgraduate year. The percentage of residents who produced at least one PubMed-indexed study during their training increased from 64.9% to 86.4% after the implementation of this research track. Residents who conducted a dedicated year of research produced significantly more publications than the categorical residents both before and after the implementation of a dual track. While a greater percentage of post-implementation categorical residents were found to have at least one PubMed-indexed publication than those before the implementation of a dual track, the differences in research productivity between these two groups were not statistically significant, as the mean publication per resident was slightly less in the DT-C cohort than the pre-DT cohort (1.4 vs 1.5, respectively). This perhaps suggests that the implementation of the research track facilitated research productivity in categorical residents who had their own interest in research without forcing it upon those residents who were less interested.
Prior studies have investigated the utility of protected research time during orthopedic surgery residency and the impact that it has on scholarly activity. Williams, Agel, and Van Heest compared the number of publications between orthopedic surgery residents who received block time, longitudinal time, and no dedicated research time.11 They reported significant differences in mean number of publications per resident across all three groups, demonstrating a correlation between both the presence and length of dedicated research time with residents’ scholarly productivity. Their results are in agreement with the findings reported in the present study. Conversely, Krueger et al. compared three orthopedic residency programs with different models of protected research time; one program with a mandatory research year, one with an elective research year, and one with no dedicated research time for residents.14 Interestingly, they found that residency programs with dedicated research time did not produce significantly more peer-reviewed publications than those without dedicated research time.
To our knowledge, our study is the first to compare scholarly output within a single orthopedic surgery program before and after the development of a dedicated research year. Valikodath et al. similarly investigated the impact of a dedicated research rotation in ophthalmology residency, with residents in their program prior to the change serving as a control group.15 They found that residents who participated in a research rotation generated more publications and presentations compared to those who had not experienced a research rotation. Papasavas et al. studied the effect of transitioning from an elective to a mandatory 2-year research track in a general surgery residency program, and reported a 3-fold increase in scientific presentations within their institution.16 Increases in scholarly productivity have been similarly reported after implementation of dedicated research time in other residencies such as internal medicine and pediatrics.17,18
The development of a research track provided our institution with a more robust infrastructure for conducting formal research that allowed us to improve scholarly activity by creating an environment where more of our residents produced peer-reviewed publications. In addition to increased scholarly output, our program benefitted from increased faculty involvement in research projects. While the addition of a research track improved our residency program, our residents also saw several benefits other than an increase in publications, as the maintenance of clinical duties during the additional research year allows residents to become more comfortable with diagnosing and managing common outpatient orthopedic conditions. Similar implementation of dedicated research tracks by other residency programs may help contribute to the development of future clinician-scientists and improve a program’s scholarly productivity.
There are several limitations to this study. It includes a relatively small sample that is only representative of residents at one institution. Additionally, by adding two residents per year, there was variation in the number of residents per year before and after implementation, though we attempted to control for this by calculating publications per residency years. Also, the overall trend toward an increased emphasis on peer-reviewed publications in the medical field may have been a contributing factor to the overall increase in resident productivity. However, there was no way to control for this, especially given the retrospective nature of this study. Furthermore, it was difficult to accurately assess other forms of research productivity such as podium and poster presentations, quality improvement projects, and other publications not indexed in PubMed. For this reason, we felt that PubMed-indexed studies were the most reliable, consistent, and accessible way to measure research productivity amongst our former residents.
Conclusions
Participating in and producing scholarly research during residency has many benefits to residents and to the field more broadly, and is an essential part of orthopedic training. An understanding of research design and methodology is essential for any orthopedic surgeon to stay current with evidence-based practice and surgical techniques. Scholarly activity also adds value to a resident’s fellowship and future career opportunities. By increasing the percentage of residents producing scholarly work at our program through the implementation of a research track, we hope our residents have reaped the benefits of having a better understanding of the research process, satisfying their academic requirements set forth by the ACGME while also becoming more competitive applicants for future fellowship and job positions. We also hope that these findings can be used to inform other programs in their decision-making around creating dedicated research time for their residents.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.