
INTRODUCTION
Upper extremity injuries account for nearly 20% of all visits to the emergency department (ED), with hand and finger fractures being the most expensive compared to all other body parts.1 The presentation rate of hand and finger injuries to the ED is 2.5 times that of the wrist or elbow, and more than 10 times that of arm injuries.2 Acute hand injuries have a significant risk of long-term functional impairment and reduced quality of life, but outcomes can be improved with prompt treatment from a specialized surgeon.1,3 Appropriate management of hand and finger injuries is thus a key component of orthopedic surgical training.
To monitor surgical exposures during training, the Accreditation Council for Graduate Medical Education (ACGME) operates a Resident Case Log System to which residents submit Current Procedural Terminology (CPT) codes after performing a procedure. Program directors can oversee clinical learning opportunities and address deficiencies in experiences. The ACGME further established guidelines in 2013 to define a threshold for the minimum number of core procedure experiences prior to graduation.4 However, the only hand-based requirement is 10 carpal tunnel releases, which is an isolated soft tissue procedure that does not accurately reflect the broad scope of orthopedic skills required for the diverse upper extremity pathology managed in independent practice.5
There is currently a paucity of literature analyzing the specific types of orthopedic hand surgery procedures logged by residents, especially pertaining to the impact of the Coronavirus Disease 2019 (COVID-19) pandemic.6–11 The primary objective of this study is to evaluate the trends in ACGME-reported hand/finger procedures reported by orthopedic surgery residents before and during the COVID-19 pandemic (2017-2022). The secondary objective is to examine trends in resident procedure logs before and after the implementation of 2013 case minimum requirements. We hypothesized that there would be a decrease in total procedures reported by residents graduating during the pandemic (academic years 2020-2021 and 2021-2022) due to cancellations of surgeries that occurred as part of national public health safety measures. We secondarily hypothesized a decrease in total procedures after implementation of ACGME case-minimum requirements due to a transition in resident reporting practices.
METHODS
Orthopedic surgery resident-reported ACGME procedure logs from the academic years of 2006-2022 (Table 1) were retrospectively reviewed. Logs were queried for adult and pediatric patients using eleven categories of hand/finger CPT codes: incision, excision, intro/removal, repair/revision/reconstruction, trauma, fracture and/or dislocation, manipulation, arthrodesis, amputation, other, and total procedures. Procedures from the trauma category (consisting of manipulation and fracture and/or dislocation categories) were only reported during 2007-2016. Microsoft Excel (Excel, Microsoft Corporation, Redmond, Washington) was used to examine and statistically analyze trends of hand procedure volumes. The unpaired 2-tailed T-test was performed to compare the logged procedure volumes before and during the COVID-19 pandemic. Trauma and other procedures were excluded due to lack of available data and low sample size of a vague category of procedures. An analysis of variance (ANOVA) was employed to compare trends of all hand/finger procedure categories. Significance for each test was set at a p-value of <0.05.
RESULTS
The number of orthopedic surgery residency programs had previously been limited to 154 during the academic years of 2017-2018 and 2019-2020 but increased to 180 in 2020-2021 and to 195 in 2021-2022. During this time, the number of residents within these ACGME-accredited programs gradually increased from 724 to 875 (Table 1). Sequential evaluation of academic years starting from the pre-pandemic control period 2017-2018 until pandemic era 2021-2022 demonstrated a continued non-significant increase in the total amount of hand/finger procedure volumes reports by graduating orthopedic surgery residents (p>0.05). After stratification by category, manipulation procedures (Figure 1) were the only ones to demonstrate a significant increase during the COVID-19 pandemic years of 2020-2021 to 2021-2022 (11.5 vs 13.2, p=0.007). No significant differences were seen in all other sub-categories of procedures when using T-tests to compare year-to-year changes during the COVID-19 pandemic (p>0.05).

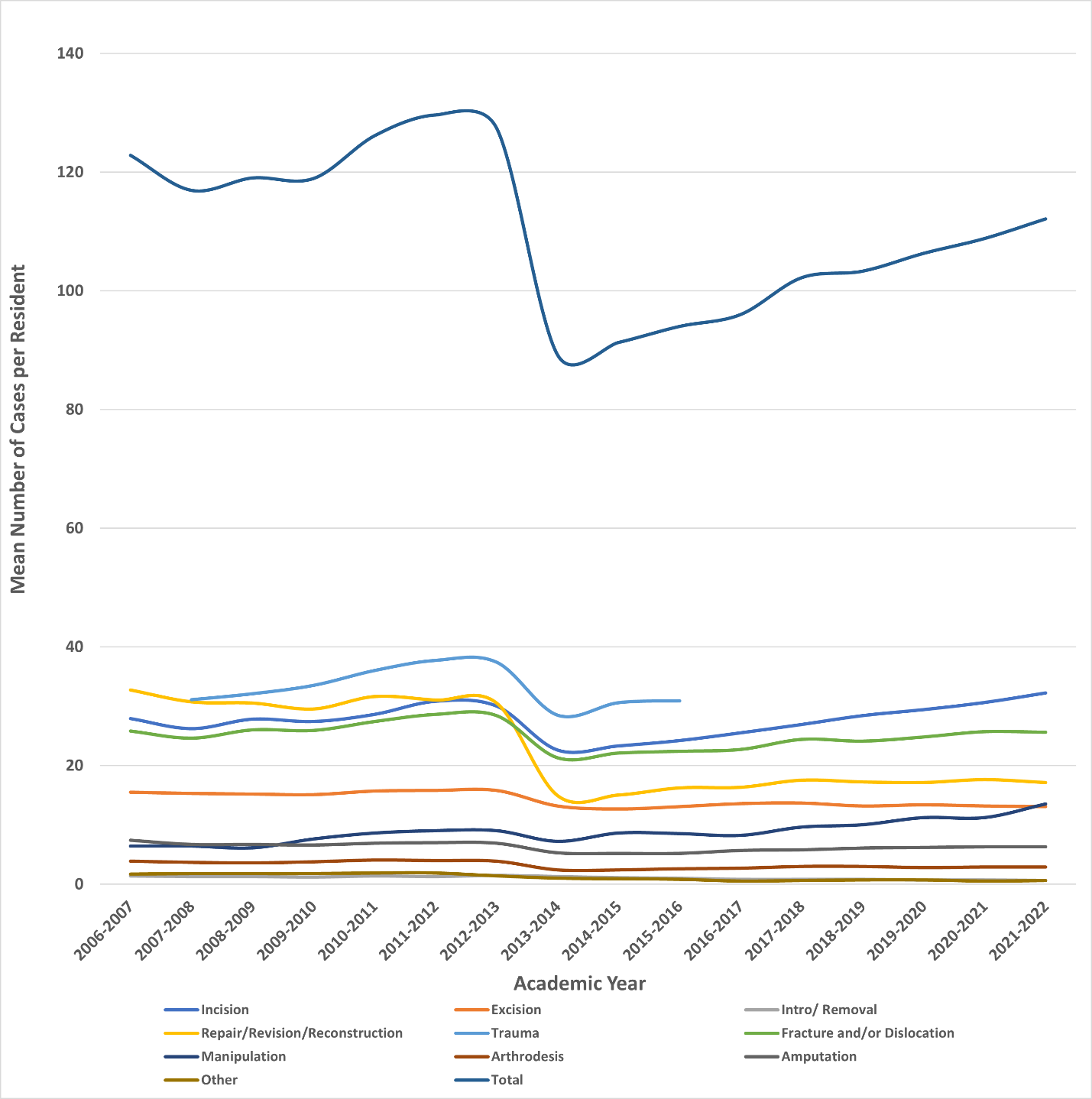
By ANOVA, there was found to be significant variation in every category from 2006 to 2022 (Table 2 and Figure 2) (p<0.0001). Compared to before implementation of case minimum requirements (2006-2013), the reported procedure volumes afterwards (2014-2022) demonstrated a significant reduction in the mean volume of hand/finger procedures per resident for incision (28.4 vs 27.0, p<0.0001), excision (15.5 vs 13.2, p<0.0001), intro/removal (1.3 vs 0.9, p<0.0001), repair/revision/reconstruction (30.9 vs 16.5, p<0.0001), trauma (34.6 vs 30.0, p<0.0001), fracture and/or dislocation (26.7 vs 23.7, p<0.0001), arthrodesis (3.9 vs 2.7, p<0.0001), amputation (6.9 vs 5.8, p<0.0001), other (1.8 vs 0.7, p<0.0001), and total procedures (123.0 vs 100.4, p<0.0001). A significant post-case minimum increase was seen in the manipulation category (7.6 vs 9.8, p<0.0001).

DISCUSSION
A retrospective review of ACGME orthopedic surgery resident hand/finger case logs from 2006-2022 revealed increasing procedure volumes, even throughout the COVID-19 pandemic. Prior to the pandemic, there was an increasing trend of adult hand/finger procedures reported by residents.7 Case volumes reported during the pandemic maintained a trend of non-significant growth, indicating that COVID-19 did not affect the amount of total hand/finger procedures performed by graduating residents. We initially hypothesized a negative trend, given that many non-urgent elective surgeries were postponed at the start of the pandemic to conserve resources for the critically ill and prevent the spread of disease.12 However, the spectrum of hand surgery uniquely consists of both elective procedures and limb-threatening emergencies requiring immediate surgery regardless of COVID status.13 Additionally, while fewer people presented with hand and finger injuries to EDs in the United States during 2020, those who did had significantly greater odds of hospitalization.14 The positive trend of procedures could reflect increased exposure to such high priority cases, even if elective procedures had slowed during the pandemic.
Hand and finger procedures can also often be performed under local or regional anesthesia, which minimizes the risk of viral aerosolization associated with intubation during general anesthesia. This, along with the increasing adoption of wide-awake local anesthesia with no tourniquet, allows for bedside treatment of localized injuries that may be associated with the increase in incision procedures.13,15 The pandemic also necessitated a more judicious selection process for surgical management. While many orthopedic conditions can be treated non-operatively, some urgent or minor procedures were performed at the bedside due to the limitations and risks of treatment in the operating room.16,17 However, these conclusions are limited, as ACGME reported data does not disclose the location of procedures or type of anesthesia used.18
Orthopedic resident logs for hand/finger procedures demonstrate the greatest variability in reported case volumes among surgical subspecialties, ranging from 10th to 90th percentile.8 Procedure log variability may be due to resident interests, suboptimal procedure logging behaviors, or sharing caseloads with plastic surgery services.8,19 Pierce et al. performed a retrospective review of orthopedic surgery resident ACGME case logs from 2010-2016 and reported that total adult hand/finger procedures had significantly decreased over this time (p<0.0001).6 Following introduction of case minimums, we also re-demonstrated a significant reduction in the mean volume of hand/finger cases per resident for total procedures. Our study further stratified these trends and found that manipulation was the only procedure category to significantly increase post-case minimum requirements (9.8 vs 7.6, p<0.0001) and has persisted during the most recent year of the pandemic (p=0.007). This supports earlier literature that demonstrated increasing clinical opportunities for manipulation of forearm/wrist fractures and improving the variability previously associated with upper extremity procedures.19,20
The implementation of new procedure log guidelines in 2013 required that just one Current Procedural Terminology (CPT) code be reported per case, even if more than one was applicable.4 Thus, logged procedures after 2013 may not accurately reflect the depth of operative experiences during this time, as there is still no consensus on how or when to separately log procedures.21 A recent study by Levidy et al. demonstrated that prior to the pandemic, there was a significant increase in adult hand/finger procedures per year from 2014-2020 (p<0.0001).7 The increasing trend prior to the pandemic could represent an adjustment to the procedure log reporting system and an improved understanding of guidelines among residency programs.18,21 A more individualized, proficiency based assessment of resident procedural skills has been suggested to improve control for ongoing variation in reporting practices.7
Limitations include our analysis based on self-reported and manually entered data directly from residents. Additionally, we did not stratify procedures by pediatric or adult procedure types and could not account for the allopathic or osteopathic-based residency programs. The procedure numbers associated with ACGME case logs are highly variable at baseline due to widespread differences in reporting practices, perceived value, and guideline interpretation by residents.18 The pandemic’s impact on procedure volume may also be underestimated, as only two complete academic years are available for analysis. Therefore, the trend of hand and finger caseloads should be followed longitudinally with a focus on determining the clinical impact of COVID-19 on orthopedic resident surgical training.
CONCLUSION
A retrospective review of graduating orthopedic surgery resident-reported ACGME hand and finger case logs from 2006-2022 revealed significant longitudinal variation in several procedure categories. Graduating orthopedic surgery residents reported increasing hand and finger procedure log volumes from 2017-2021, and demonstrated a maintained, but non-significant, growth in volume during the COVID-19 pandemic.