




BACKGROUND
Art-based learning has been recognized as an important element in the educational program of medical students and residents in training.1–3 Several studies have shown enhancement of observational skills and social competencies through examining visual arts.4,5 A museum provides an excellent setting for observational training as it combines a fine collection of art works with an inspiring environment.6
Surgery largely depends on visual assessment of physical findings and diagnostic imaging necessary to consider a surgical intervention, in conjunction with patients’ conditions and preferences.7 In particular in the OR, visual recognition of an anatomical situation and visual guidance of manual movements are paramount in performing an operation, whether in open surgery or in endoscopic procedures undertaken laparoscopically or robot-assisted. Eye-hand coordination is key in operative surgery and starts with critical observation. Training the eye therefore, is as important in surgical education as training of manual skills.
In collaboration with the Rijksmuseum in Amsterdam, we have set up an art-based course for medical students and surgical residents in our institution, the Amsterdam University Medical Center.8 Focusing on observational training and group discussion, we devised a method to facilitate structured observation of an art work with ultimately, recognition of a possible physical abnormality shown in the work, thereby translating observational findings to a diagnosis. This led to the ABCD method in providing a template for medical students and surgical residents to critically observe and discuss a series of art works, selected on the basis of a medical feature detected on careful examination of the picture. The ABCD-method is based on ‘observing-in-layers’ (ABC) to which a diagnostic (D) aspect was added, discussing the image in a medical context. We aimed to evaluate application of the ABCD-method in a series of art-based workshops conducted in the Rijksmuseum for medical students and surgical residents.
METHODS
Program design
Our program ‘See better, by looking at art’ was devised through collaboration of the surgical department of the Amsterdam University Medical Center and the art educational department of the Rijksmuseum in Amsterdam.8 The Rijksmuseum is one of the top museums in the Netherlands, famous for its unique collection of art works, spanning periods from the Middle Ages to modern and contemporary art. Medical students and surgical residents enrolled in an interactive workshop focused on art observation facilitated by an art-educator and a surgeon (TvG) who guided the group as tutors. The learning objectives have been reported previously.8 The program was evaluated in a post-workshop survey focusing on valuation and contribution of the course to professional development. The survey comprised a questionnaire consisting of ‘open’ questions regarding various aspects and learning objectives of the program as previously described.8
The ABCD-method
The ABCD-method refers to four stages in viewing an art work, set on the basis of ‘observing-in-layers’ and a group discussion (Table 1). A stands for ‘attention’ to start out; ‘take your time’ and concentrate on what you see, spend one minute on carefully looking at the image. The B stands for ‘behold’, the next part of looking at an object; name the objects that stand out, describe how the objects are inter-connected, discover the context of the composition and try to come to an interpretation of the work as conveyed by the artist. The C is of ‘communication’, the way we connect with each other in exchanging thoughts generated by what we have seen and in sharing what is experienced in the group. Finally, the D stands for ‘diagnosis’ and draws attention to a medical aspect shown, that can be associated with an abnormal physical feature of a person depicted or with medical concepts at the time of the work. This is what could be called the ‘iconodiagnostic’ part of the session, associating iconographical information with a medical condition.
Content of workshops and participants
Workshops consisted of a 2-hour tour through the museum passing by 8-10 works of art. The groups consisted of 6-12 participants, of different levels of education and experience, mainly medical students, residents and doctors. Participants were engaged in exercises during the workshop to train their observational skills.8 At the end of the tour, the group would come together for evaluation and completion of the survey.
Two groups of participants were considered: In the first group (group I) participants enrolled from August 2021 to May 2023 (with a 1 year break in between because of COVID-19 restrictions). This group followed the initial structure of the art-based medical education program developed in collaboration with the Rijksmuseum, focusing on observational and communicational skills, corresponding with the A,B and C of the ABCD-method. As per recommendation of the first group, a medical aspect was included in the following workshops. Hence, from December 2023 to March 2024, all participants received the complete ABCD-method, comprising group II.
Selection of art works
Paintings or sculptures were selected from the vast collection of the Rijksmuseum on permanent display. A choice was made by the authors and art-educators of the Rijksmuseum on the basis of visual suitability for a group, art-historical content and a medical feature depicted. Associations with medical conditions or abnormalities were confirmed by consensus among various specialists in specific fields; general surgery, plastic surgery, orthopedic surgery, internal medicine, neurology, psychiatry, dermatology, pediatrics, gynecology and obstetrics.
RESULTS
Participants and art works
In all, 128 participants including medical students, medical PhD students, surgical residents and certified surgeons joined the workshops. In group I, 63 participants enrolled joining in 9 workshops. After adding a diagnostic element to the program, 65 participants followed the complete ABCD-method in 11 workshops (group II).
The art works visited were paintings and sculptures predominantly from the Renaissance or Baroque periods, all listed in the catalogue of the Rijksmuseum.9
Evaluation of the ABCD-method
After 1-2 minutes of attention and close examination of a work of art (part A of the method), the participants continued with part B of the workshop, encompassing three steps of observation: Participants in turn, named an object or feature observed in the art work, described relationships between items, and finally formulated an interpretation of the work. Then, a group discussion followed (part C, communication) in which thoughts were exchanged leading to a balanced conclusion, as paraphrased by the guide and clinician. The process of postponing judgement until all views were discussed, clearly unfolded in the group. Finally, detectable physical abnormalities in the art work were noted from the perspective of possible clinical conditions and discussed. This led to a putative clinical diagnosis (part D).
Evaluation of the exercises undertaken in the workshops
Three sorts of exercises contained in the program, were undertaken by the participants in both groups I and II.
-
Drawing from memory
This exercise included observing a painting for one minute after which participants were asked to turn around and draw the picture they had seen from memory on a sheet of paper. The sketches were discussed in the group, emphasizing the main points reproduced from the painting and the side points. How was the painting framed, mounted in a square or rectangular frame, or in a round frame (a tondo). Were all the subjects depicted reproduced in the sketches of the participants. Which details in the picture were noted and which were of less importance. This exercise targeted at memorizing the main points (of a patient) and leaving out details that are not relevant to the case. -
Seeing through someone else’s eyes
In an exercise, entitled ‘Seeing through someone else’s eyes’, the participants turned their back to a piece of art while one participant was instructed to describe the artwork to the others. Based on the description they received, the participants were asked to draw the picture on a sheet of paper. The sketches were placed side by side and discussed in the group in face of the actual work of art. The disparate interpretations of the transmitted information became apparent in the resulting sketches, showing the differences between observations of the describer and interpretations of the receivers. This is recognized in clinical practice when rendering information regarding patients among colleagues. -
Embodiment
In this exercise, named ‘embodiment’, a participant described the posture of a sculptured subject to a partner who was blinded to the sculpture. According to the bodily information, the listener would take the stand and posture represented by the sculpture. Photographs were taken using smartphones and compared with the sculpture. This exercise requires translating someone else’s instructions into one’s own physical perception.
Evaluation of iconodiagnostics
Iconodiagnostics added a medical stance in observing the artworks. Most of the paintings or sculptures that were selected, revealed a component that could be associated with a medical condition, according to features depicted by the artists, whether intended or by coincidence. These associations were obviously made on the basis of visual elements in the work of art as recognized from known clinical attributes, as outlined by the senior clinician.
A series of putative diagnostic conclusions were considered ranging from neonatal macrosomia, to goitre and Cushing’s syndrome. Three of the latter art works are elaborated here, showing the alleged abnormalities and possible diagnostic inferences. These medical connotations to our knowledge, have not been noted or reported before in relation with the discussed artworks.
Erb’s palsy
The painting shown in fig 1, is entitled ‘The well-stocked kitchen’ and was made in 1566 by Joachim Bueckelaer, a Flemish artist from Antwerp. In the foreground, an abundance of food is displayed, vegetables, fruit and poultry. The background, on some distance shows Jesus in the house of Martha and Mary, as is the theme of this painting taken from the eponymous story of the New Testament.
._.jpeg)
).jpg)
An elderly man is seen half-way in the background, whose left arm is underdeveloped resting with the hand on his thigh. The arm is rotated internally, the forearm extended and pronated with the wrist and fingers flexed. The posture of the limb, also referred to as ‘Waiter’s tips posture’, is characteristic for Erb’s palsy typically caused by injury to the brachial plexus at birth.10 (see inset of fig 1)
The atrophic appearance and posture of the left arm was not often recognized by the participants. The association with Erb’s paralysis was noticed when a participant happened to have encountered such a case during clinical rounds. One participant recognized the deformity as she had a friend who still needed a brace because of the injury acquired at birth. Another mentioned that Kaiser Wilhelm II of Germany had contracted left brachial plexus palsy because of birth trauma, usually carefully concealed underneath his clothing.11 A third participant remarked that the film actor Martin Sheen (of Apocalypse Now) also had Erb’s paralysis of his left arm.
Neglected congenital clubfoot
‘The Seven works of Mercy’ consists of seven panels depicting compassionate acts to help those in need in a Dutch city in 1504 (artist unknown).12 On one of the panels, a disabled man is seen resting on the street with both legs flexed in the hips and stretched in the knees. (fig 2) He apparently is unable to walk and moves forward using hand crutches. Both his feet are rotated inwards and downwards (equinovarus position) and remarkably, his left foot is depicted with seven toes. (see inset of fig 2) The foot deformity is compatible with congenital clubfoot while the combination with two extra toes (polydactyly) suggests an underlying genetic disorder known as Trisomy 13 (Patau Syndrome).13 The fact that he is unable to stand or walk may alternatively suggest a combination with upper motor neuron paralysis. These considerations generated a lively discussion among the participants and the senior clinician.

).jpg)
Isolated accessory nerve injury
A wooden sculpture of a boy sitting in a pot (around 1500, anonymous) represents Vitus, who evidently is in anguish. Vitus was a 4th-century Sicilian boy who converted to Christianity and for that, was severely punished by the pagans. He was tortured and thrown in a pot with boiling oil, resin and pitch. Despite these torments, he remained faithful to his belief and miraculously survived. Because of his courage and faith as a martyr, he was declared a saint by the Christian Church. The sculpture shows the boy with a sloping right shoulder while his hands are folded in prayer. (fig 3) He is looking downwards with his head slightly turned to the left. The physical appearance of the lower right shoulder suggests paralysis of the ipsilateral trapezius muscle. This can result from injury of the accessory nerve, the 11th cranial nerve that innervates the trapezius and sternocleidomastoid muscles, as may occur after trauma to the neck or base of the skull.14 The posture of his head can fit with dysfunction of the right sternocleidomastoid muscle limiting lateral flexion of the head to the same side and rotation of the head to the left.

The sculpture of Saint Vitus was the subject in the exercise ‘Seeing through someone else’s eyes’ described above. One participant was instructed to describe the artwork while the others with their backs to the sculpture, could not see the subject. They drew what they perceived from the description of the describer. The position of the right shoulder was oftentimes not noted by the describer and therefore, not reproduced by the sketcher. The discussion resulted in reappraisal of the anatomy and function of the muscles of shoulder and the neck and showed how clinical signs can be missed in a handover.
Outcomes of the post-workshop surveys
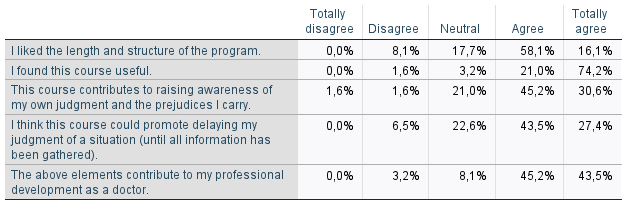
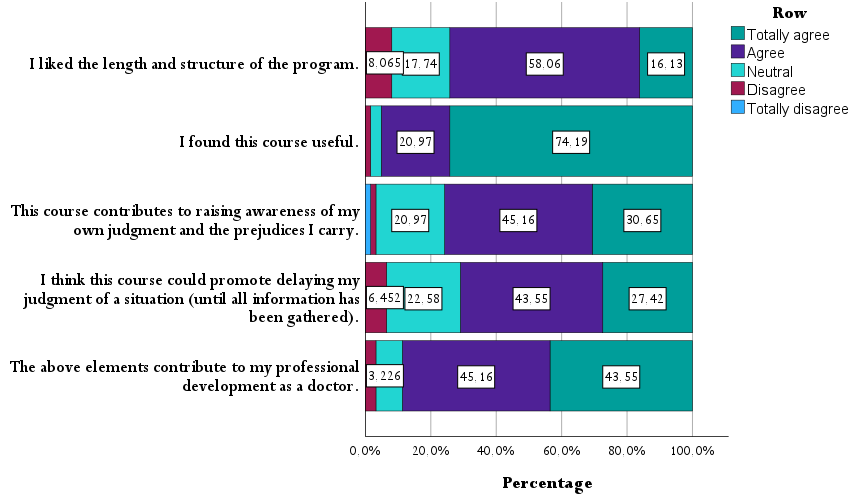
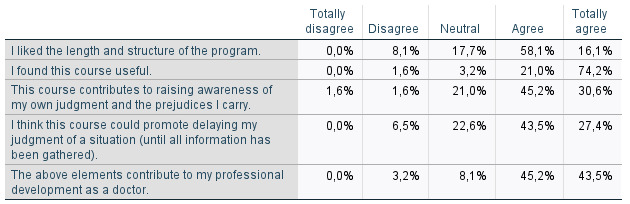
Of all questionnaires sent out to the 128 participants after the workshops, 127 lists were returned (response rate. 99%). The ratings of the program as evaluated through the surveys in group I (n=62) are shown in table 2. Overall, the participants were enthousiastic about the format and content of the workshops, scoring high in all domains.
Adding up the positive scores ‘agree/totally agree’, the proportions listed for ‘length and structure’, ‘usefulness’ and ‘contribution to professional development’, were 74.2%, 95.2% and 88.7%, respectively.

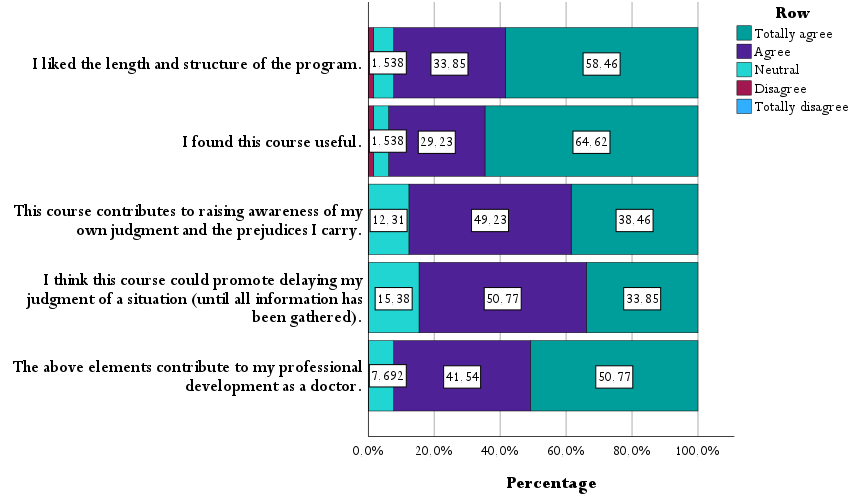
The ratings listed in group II (n=65) in which the complete ABCD-method was applied, are shown in table 3. The proportions listed for ‘length and structure’, ‘usefulness’ and ‘contribution to professional development’ in group II, were 92.3%, 93.8% and 92.3%, respectively.
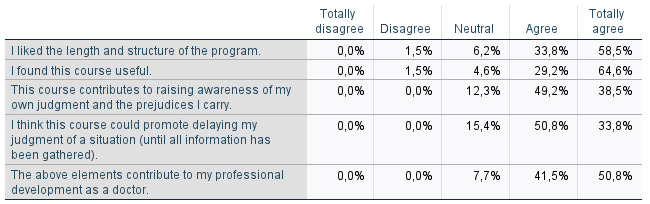

Although the participants of group II had not experienced a workshop without the diagnostic part preventing direct comparison of the groups, the ratings show an overall increase in group II.
DISCUSSION
Learning how to observe and describe is key in our professional education. These competences go beyond physical examination only, and are crucial in recognizing emotions and empathizing with patients.15 Developing ‘visual literacy’ is especially important in surgery, as diagnostic and operative skills largely rely on visual information and interpretation. Although the added value of art-based medical education is increasingly recognized in the Netherlands, art-based programs greatly vary among the medical faculties and mostly depend on institutional facilities and local art museums.16 Art-based learning has up to now not been part of surgical training programs in the Netherlands.
We set-up a course with the Rijksmuseum in Amsterdam to offer our medical students and surgical residents structured training in observational skills, by looking at art objects in the museum.8 The key elements of such a program are three-fold: to look carefully, to verbalize what is seen but delay judgment, and finally, to interact with others regarding interpretations and meaning.15 The workshop was based on ‘observing-in-layers’ in which participants standing in front of a painting, were first asked to carefully observe the items, persons or objects on the canvas. In three steps, the observed items or features are named, described in their depicted connection and finally discussed in the group in regard with the presumed meaning of the composition by the artist. The role of the tutors was to guide the discussion and paraphrase the comments, at this point following the lines of Visual Thinking Strategies (VTS).5,6,16 This approach laid the basis of the A, B and C as subsequently integrated in the ABCD-method.
Both students and residents were enthusiastic about the course in the museum and recognized the value of art-based observational training for their professional development. A frequently heard comment however, was that concomitant teaching of a medical entity would enhance the impact of the program. Discussing a medical condition in relation with an art work, would particularly satisfy the medical students, eager to learn from a ‘clinical picture’. Amazed by the number of works in the abundant collection of the Rijksmuseum in which we discovered an abnormal physical feature or an associated medical aspect, we decided to include a selection of these art works in our course. The addition of a diagnostic element in our approach, represented by the D in our ABCD-method, was very much appreciated as conveyed by the participants.
A number of artworks with a medical connotation was discussed in the workshops, of which three have been described above, all masterpieces of 16th century artists. Of course, the question arises whether the physical features we associated with medical conditions, were depicted by the artists as realistic features appearing in their subjects, or that resemblance was coincidental. Several Renaissance painters tended to reproduce what they saw in a realistic form and copied physical details even if these were not very attractive or did not add to the beauty of their live model.17,18 Hence, any bump, pimple or deformity was depicted as real.
For an image as shown in figure 2, there is little doubt that the depicted foot deformity matching clubfoot in combination with 7 toes (polydactyly), was a realistic representation by the artist of a person with this congenital deformity. The same can be said of the atrophic left arm of the person shown in figure 1 in a posture typical of Erb’s paralysis. The sloping shoulder and slightly rotated head of the boy presented in the sculpture shown in fig 3, however, could be an artistic touch made by the artist to emphasize the miserable condition of the boy in the pot. Notwithstanding this ambiguity, the description and explanation by an experienced clinician pointing out characteristic physical features, was experienced as instructive and useful.
The conducted surveys, although providing subjective data on a semi-quantitative basis, offered insight into how the program was received. All participants, irrespective of their grades or professional level, highly valued the set-up and content of the course. The environment of the museum offered a welcome change to the usual hospital walls and lecture halls, clearly enhancing satisfaction with the workshops, both on the part of the participants as the accompanying medical educators. Inclusion of a diagnostic element opened up a medical perspective in the program that proved instructive especially for the medical students. What stood out was the interaction among the participants with lively narratives and discussions creating cohesion within the group. In terms of team-building, the workshops in the museum provided an excellent option.
Art-based learning has not been widely adopted in surgical training programs, while various skills-lab courses are available to train residents in surgical techniques, such as the training modules in laparoscopic surgery. ‘Training the eye’ in the art museum along the same lines, deserves a place in surgical training offering several benefits in an inspiring environment. In most of the larger cities worldwide, there are fine art museums with collections suitable for local art-based workshops using the ABCD-method, although that requires prior scrutiny of the collection and selection of the objects available. We have initiated similar art-based courses with surgical departments in Rotterdam (Erasmus Medical Center) and The Hague (Haaglanden Medical Center), in collaboration with Museum Boijmans Van Beuningen and Museum Mauritshuis, in Rotterdam and The Hague, respectively.
A hurdle in proposing art-based initiatives in educational programs is the lack of validated tools to assess the added value of these courses in terms of observational competences and cognitive functions.19 A challenge for the future is therefore, to develop these tests to quantitatively assess observational skills in a standardized fashion, possibly with inclusion of a control group. A way to go is to engage several surgical departments and training centers nationwide in art-based courses using the same set-up and methods, enabling coordinated assessment of art-based observational training in larger numbers of participants.
CONCLUSION
We devised an art-based educational course in the Rijksmuseum in Amsterdam offering observational training for medical students and surgical residents using art objects displayed in the museum. We introduced the ABCD-method to structure the process of close observation and group discussion in workshops, including a medical, diagnostic feature. A series of medical conditions was delineated according to physical abnormalities conceived in the artworks. Post-workshop evaluation of the program showed overall, highly positive ratings of the course in the vast majority of participants.
Acknowledgement
We wish to thank Pauline Kintz of Rijksmuseum, Amsterdam, The Netherlands, for her collaboration in our educational project.